

Population-wide analysis of differences in disease progression patterns in men and women
- PMID: 30737381
- PMCID: PMC6368599
- DOI: 10.1038/s41467-019-08475-9
Population-wide analysis of differences in disease progression patterns in men and women
Abstract
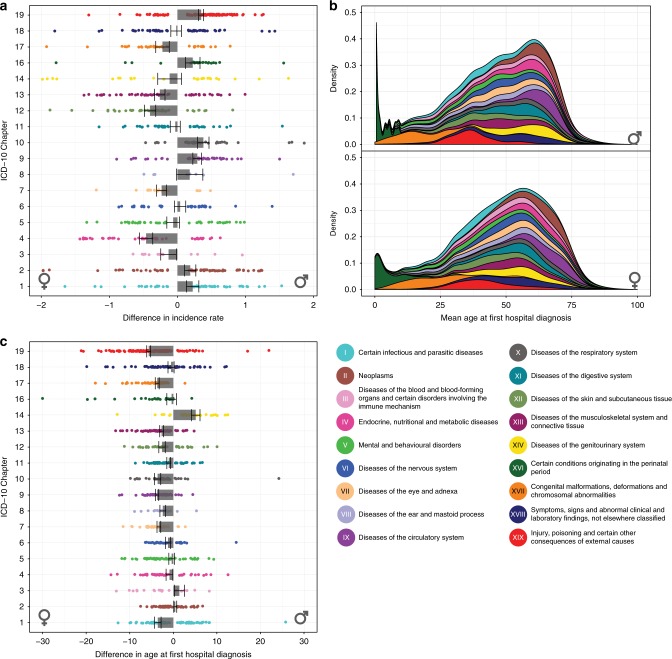
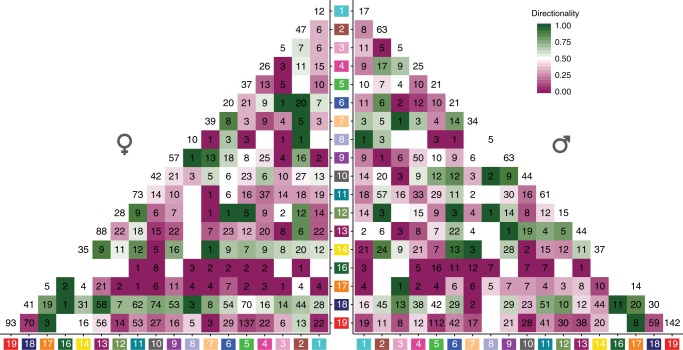
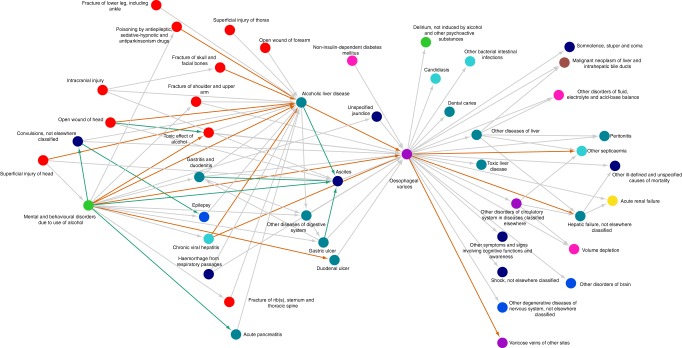
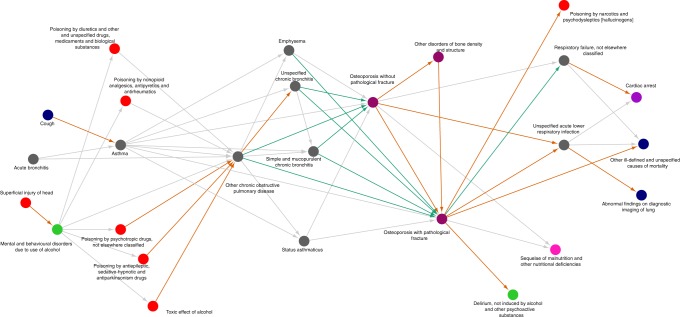
Sex-stratified medicine is a fundamentally important, yet understudied, facet of modern medical care. A data-driven model for how to systematically analyze population-wide, longitudinal differences in hospital admissions between men and women is needed. Here, we demonstrate a systematic analysis of all diseases and disease co-occurrences in the complete Danish population using the ICD-10 and Global Burden of Disease terminologies. Incidence rates of single diagnoses are different for men and women in most cases. The age at first diagnosis is typically lower for men, compared to women. Men and women share many disease co-occurrences. However, many sex-associated incongruities not linked directly to anatomical or genomic differences are also found. Analysis of multi-step trajectories uncover differences in longitudinal patterns, for example concerning injuries and substance abuse, cancer, and osteoporosis. The results point towards the need for an increased focus on sex-stratified medicine to elucidate the origins of the socio-economic and ethological differences.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Franconi, F., Sanna, M., Straface, E., Chessa, R. & Rosano, G. Sex and Gender Aspects in Clinical Medicine. Pathophysiology (Springer, New York, 2012).
-
- World Health Organization. WHO gender policy: integrating gender perspectives in the work of WHO. http://origin.who.int/gender-equity-rights/knowledge/a78322/en/ (Accessed 22 February 2018). (2002).
