

Complex karyotype in de novo acute myeloid leukemia: typical and atypical subtypes differ molecularly and clinically
- PMID: 30737482
- PMCID: PMC6609457
- DOI: 10.1038/s41375-019-0390-3
Complex karyotype in de novo acute myeloid leukemia: typical and atypical subtypes differ molecularly and clinically
Abstract
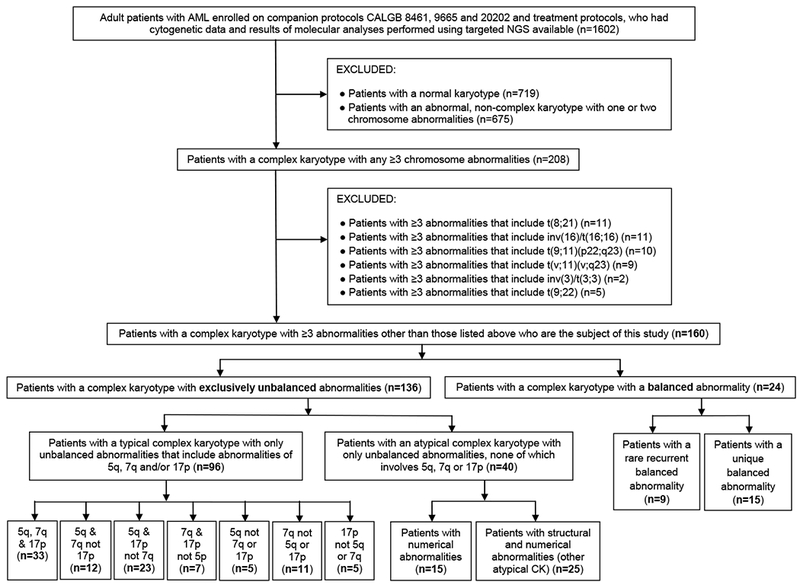
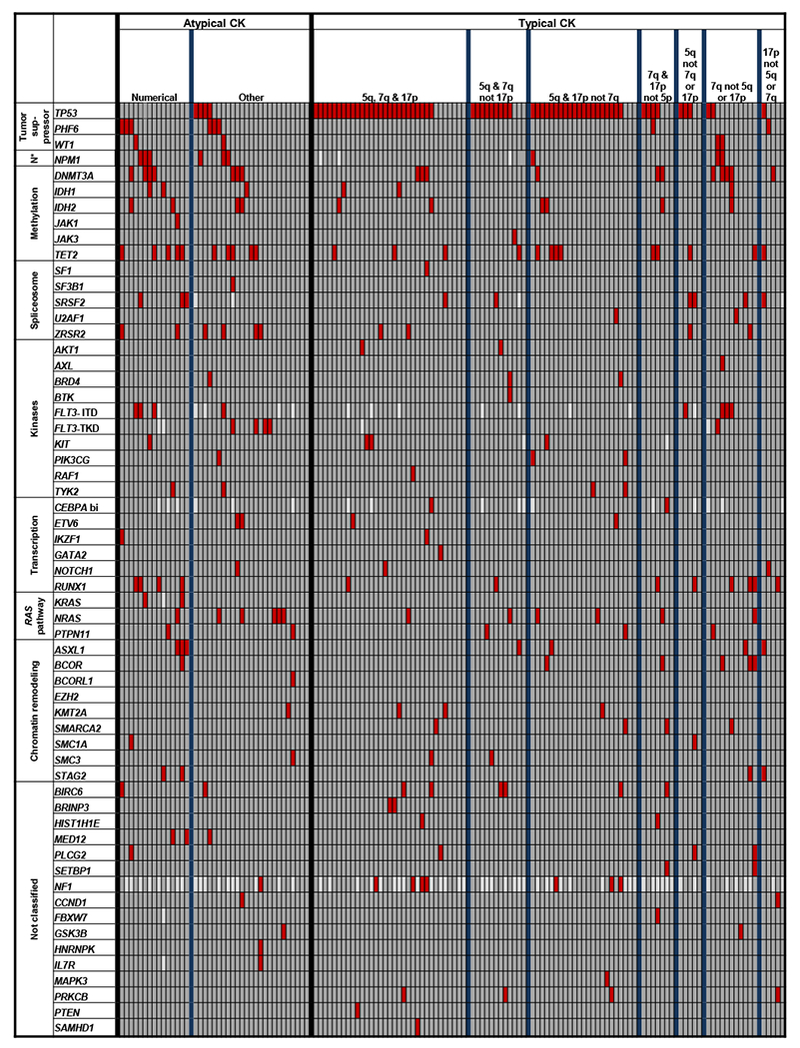
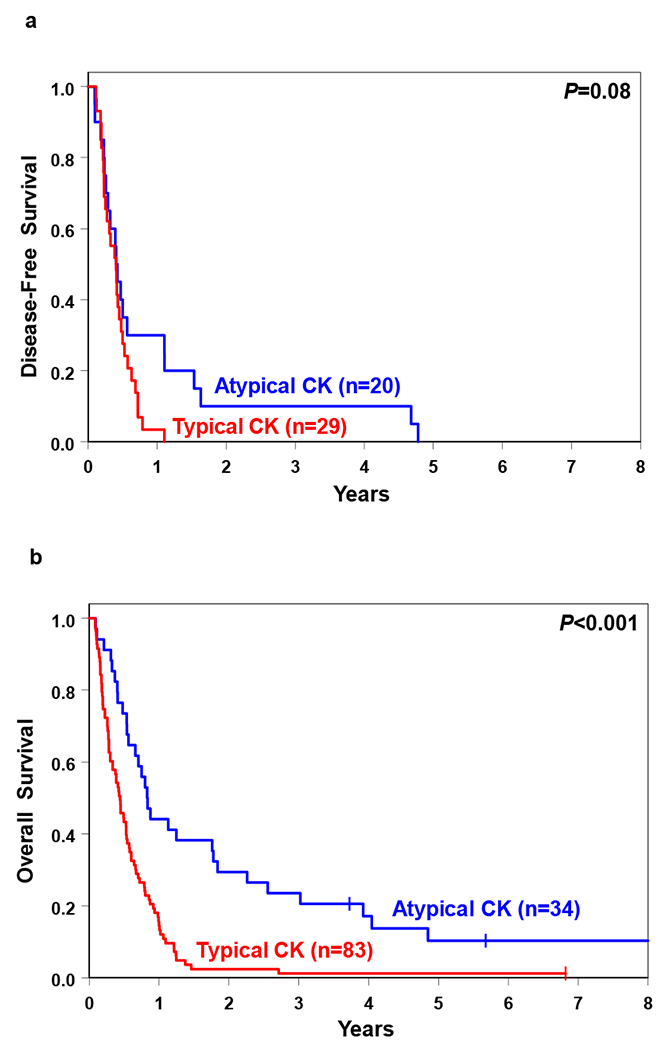
Complex karyotype (CK) with ≥ 3 abnormalities is detected in 10-12% of patients with acute myeloid leukemia (AML) and associated with poor prognosis. The most common unbalanced abnormalities found in CK result in loss of material from the 5q, 7q, and/or 17p chromosome arms. The presence of 5q, 7q, and/or 17p abnormalities denotes typical CK and their absence denotes atypical CK. Since molecular features of CK-AML are not well characterized, we investigated mutational status of 81 leukemia/cancer-associated genes in 160 clinically well-characterized patients. They included 136 patients with ≥ 3 exclusively unbalanced chromosome abnormalities, 96 of whom had a typical CK and 40 atypical CK, and 24 patients with ≥ 1 balanced abnormality in addition to ≥ 2 unbalanced ones. Patients with atypical CK-AML differed from those with typical CK-AML: they carried TP53 mutations less often (P < 0.001) and more often PHF6 (P = 0.008), FLT3-TKD (P = 0.02), MED12 (P = 0.02), and NPM1 (P = 0.02) mutations. They were younger (P = 0.007), had higher WBC (P = 0.001) and percentages of marrow (P < 0.001) and blood (P = 0.006) blasts, higher complete remission rates (P = 0.02), and longer overall survival (P < 0.001), thus indicating that atypical and typical CK-AMLs constitute distinct disease subtypes. We also identified smaller patient subsets within both typical and atypical CK-AML that differed molecularly and clinically.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Mrózek K, Heerema NA, Bloomfield CD. Cytogenetics in acute leukemia. Blood Rev 2004; 18: 115–136. - PubMed
-
- Byrd JC, Mrózek K, Dodge RK, Carroll AJ, Edwards CG, Arthur DC et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461). Blood 2002; 100: 4325–4336. - PubMed
-
- Schoch C, Haferlach T, Haase D, Fonatsch C, Löffler H, Schlegelberger B et al. Patients with de novo acute myeloid leukaemia and complex karyotype aberrations show a poor prognosis despite intensive treatment: a study of 90 patients. Br J Haematol 2001; 112: 118–126. - PubMed
-
- Slovak ML, Kopecky KJ, Cassileth PA, Harrington DH, Theil KS, Mohamed A et al. Karyotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group study. Blood 2000; 96: 4075–4083. - PubMed
-
- Farag SS, Archer KJ, Mrózek K, Ruppert AS, Carroll AJ, Vardiman JW et al. Pretreatment cytogenetics add to other prognostic factors predicting complete remission and long-term outcome in patients 60 years of age or older with acute myeloid leukemia: results from Cancer and Leukemia Group B 8461. Blood 2006; 108: 63–73. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA077658/CA/NCI NIH HHS/United States
- P30 CA016056/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U10 CA101140/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- UG1 CA233191/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA180866/CA/NCI NIH HHS/United States
- P50 CA140158/CA/NCI NIH HHS/United States
- U10 CA180861/CA/NCI NIH HHS/United States
- UG1 CA233331/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- UG1 CA233338/CA/NCI NIH HHS/United States
- U24 CA196171/CA/NCI NIH HHS/United States
- P30 CA016058/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
