

The Diagnosis and Blistering Mechanisms of Mucous Membrane Pemphigoid
- PMID: 30740099
- PMCID: PMC6357922
- DOI: 10.3389/fimmu.2019.00034
The Diagnosis and Blistering Mechanisms of Mucous Membrane Pemphigoid
Abstract
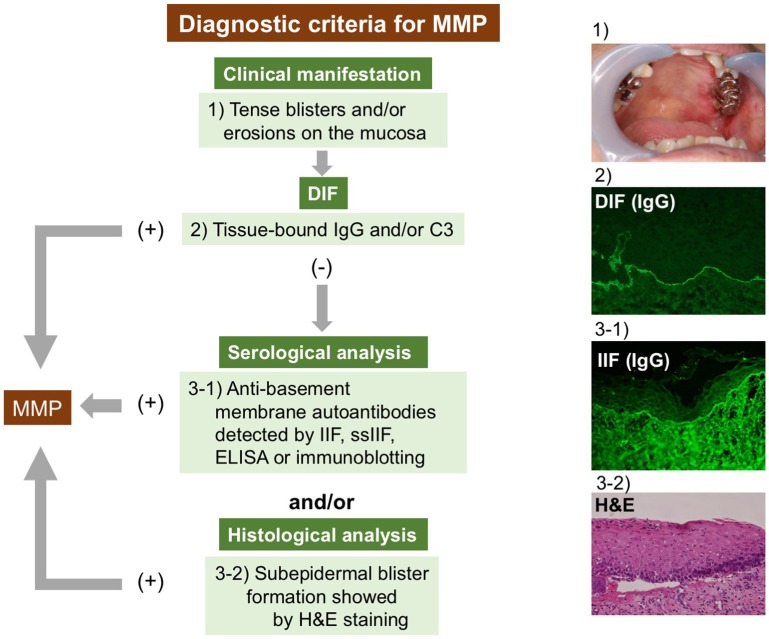
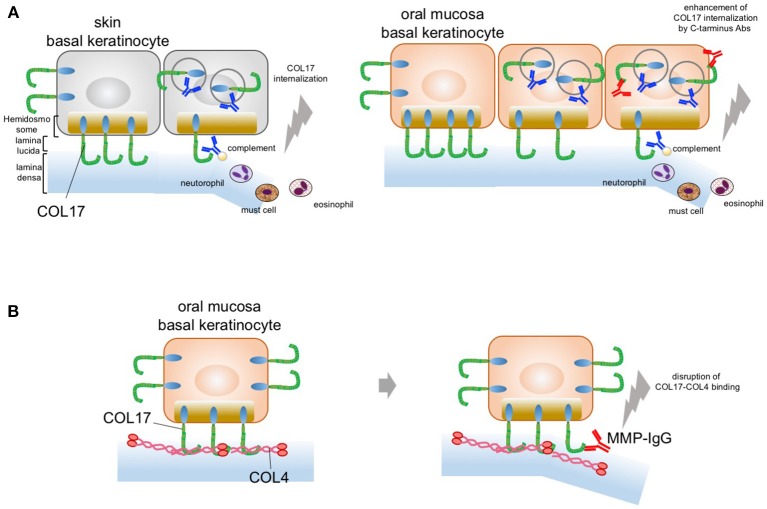
Mucous membrane pemphigoid (MMP) is a mucous membrane-dominated autoimmune subepithelial blistering disease that is caused by autoantibodies against various autoantigens in basement membrane zone (BMZ) proteins, including collagen XVII (COL17). Clinicians face diagnostic problems in detecting circulating antibodies and targeted antigens in MMP. The diagnostic difficulties are mainly attributed to the low titers of MMP autoantibodies in sera and to heterogeneous autoantigens. Additionally, no unanimous diagnostic criteria have been drawn for MMP, which can result in delayed diagnoses or misdiagnoses. This review aims to integrate and present currently available data to clarify diagnostic strategies and to present diagnostic criteria for MMP. The ultimate blistering mechanism in MMP has not been elucidated, and such mechanism is especially obscure in COL17-type MMP. In bullous pemphigoid (BP), which is the most common autoimmune subepidermal blistering disease, some patients show oral lesion as well as predominant skin lesions. However, there is no fundamental explanation for the onset of oral lesions in BP. This article summarizes innovative research perspectives on the pathogenesis of oral lesions in pemphigoid. Finally, we propose a potential pathogenesis for COL17-type MMP.
Keywords: C-terminas; collagen IV; direct immunofluorescence; mucous membrane pemphigoid; steric hindrance; type XVII collagen.
Figures
References
-
- Chan LS, Ahmed AR, Anhalt GJ, Bernauer W, Cooper KD, Elder MJ, et al. . The first international consensus on mucous membrane pemphigoid: definition, diagnostic criteria, pathogenic factors, medical treatment, and prognostic indicators. Arch Dermatol. (2002) 138:370–9. 10.1001/archderm.138.3.370 - DOI - PubMed
-
- Schmidt E, Skrobek C, Kromminga A, Hashimoto T, Messer G, Bröcker EB, et al. . Cicatricial pemphigoid: IgA and IgG autoantibodies target epitopes on both intra- and extracellular domains of bullous pemphigoid antigen 180. Br J Dermatol. (2001) 145:778–83. 10.1046/j.1365-2133.2001.04471.x - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical