

Targeting Tregs in Juvenile Idiopathic Arthritis and Juvenile Dermatomyositis-Insights From Other Diseases
- PMID: 30740105
- PMCID: PMC6355674
- DOI: 10.3389/fimmu.2019.00046
Targeting Tregs in Juvenile Idiopathic Arthritis and Juvenile Dermatomyositis-Insights From Other Diseases
Abstract
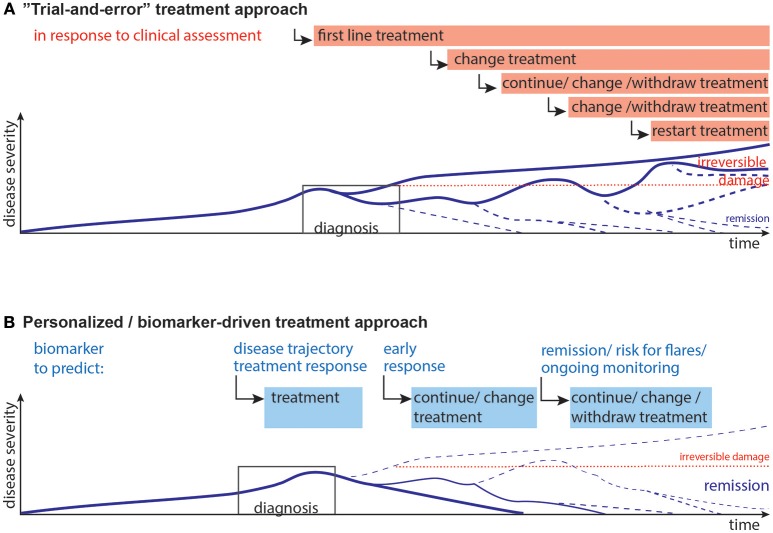
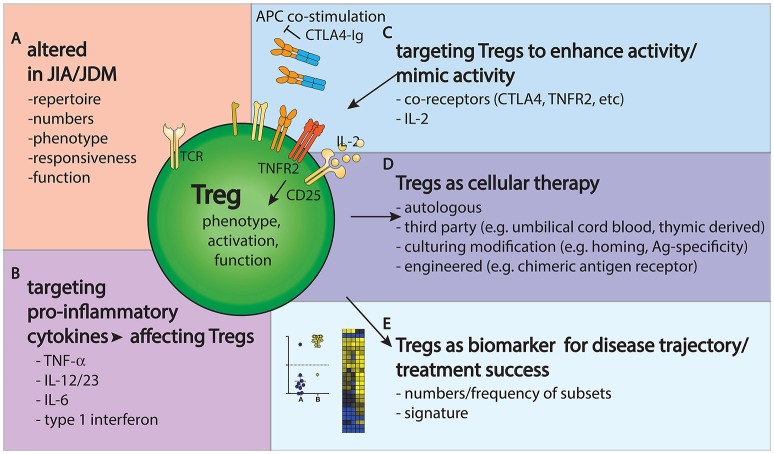
Regulatory T cells (Tregs) are believed to be dysfunctional in autoimmunity. Juvenile idiopathic arthritis (JIA) and juvenile dermatomyositis (JDM) result from a loss of normal immune regulation in specific tissues such as joints or muscle and skin, respectively. Here, we discuss recent findings in regard to Treg biology in oligo-/polyarticular JIA and JDM, as well as what we can learn about Treg-related disease mechanism, treatment and biomarkers in JIA/JDM from studies of other diseases. We explore the potential use of Treg immunoregulatory markers and gene signatures as biomarkers for disease course and/or treatment success. Further, we discuss how Tregs are affected by several treatment strategies already employed in the therapy of JIA and JDM and by alternative immunotherapies such as anti-cytokine or co-receptor targeting. Finally, we review recent successes in using Tregs as a treatment target with low-dose IL-2 or cellular immunotherapy. Thus, this mini review will highlight our current understanding and identify open questions in regard to Treg biology, and how recent findings may advance biomarkers and new therapies for JIA and JDM.
Keywords: biomarker; juvenile dermatomyositis; juvenile idiopathic arthritis; regulatory T cells; therapy.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical