

Risk factors for complications and adverse outcomes in polytrauma patients with associated upper extremity injuries
- PMID: 30740144
- PMCID: PMC6360674
- DOI: 10.1186/s13037-019-0187-3
Risk factors for complications and adverse outcomes in polytrauma patients with associated upper extremity injuries
Abstract
Background: In terms of upper extremity fractures by patients with multiple injuires, a lot of studies have assessed the functional outcome following trauma to have less favorable outcomes in regards to functional recovery. We tested the hypothesis that differences in clinical outcome occur between shaft and articular injuries of the upper extremity, when patients that sustained neurologic deficits (e.g. brachial plexus lesions) are excluded.
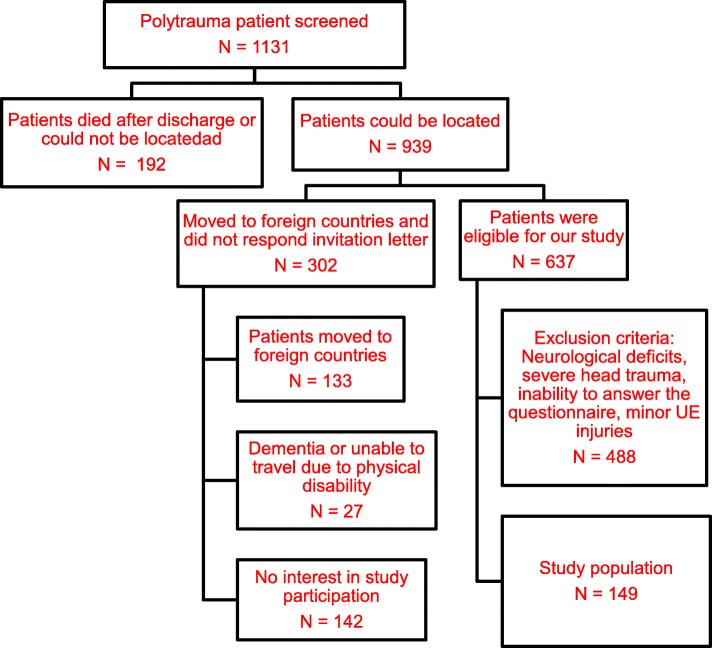
Methods: We involved Patients with isolated or combined upper extremity fracture, ISS > 16 in a level one trauma center. The follow up was at least 10 years after the initial injury. Both clinical examination (range of motion, instability, contractures, peripheral nerve damage) and radiographic analysis were carried out. We evaluated also the development of heterotopic ossifications. To analyse patients were subdivided into 3 different subgroups (articular [IA], shaft [IS], and combined [C]).
Results: A statistically significant difference was found when ROM was compared between Group IS and C (p = 0.012), for contractures between Groups IA and C (p = 0.009) and full muscle elbow forces between Groups IS and C (p = 0.005) and Group IA and IS (p = 0.021). There was a significantly increased incidence in heterotopic ossifications when articular involvement was present. This applied for the isolated (p < 0.02) and the combined group (Group C vs Group IS, p = 0.003).When Brooker type I/II in group IA and Brooker types III/IV were combined, there was a significant difference (p < 0.001). In group IA (n = 1) and in group C (n = 6), HO developed or worsened after revision surgery, all of which were performed for malunion or nonunion.
Conclusions: In this study, patients with isolated shaft fractures of the upper extremity tend to have a more favorable outcome in comparison with combined to isolated articular fractures in terms of range of motion, pain and the ability to use the arm for everyday activities.In the clinical practice of the treatment of polytraumatized patients with upper extremity injuries, we feel that the relevance of these injuries should not be underestimated. They are especially prone to development of heterotopic ossifications, thus requiring prophylactic measures, if necessary. As their incidence increases with the rate of reoperations, we feel that even during initial care, meticulous surgery is required to avoiding the necessity of revision surgeries. Similar to injuries below the knee, upper extremity injuries, should be treated to avoid any functional disability.
Keywords: Articular fracture; Heterotopic ossification; Multiply injured patient; Upper extremity fracture.
Conflict of interest statement
The study was approved by the local Institutional Review Board and the local Medical Ethical Committee (University Hospital Zurich). General consent was obtained according to the institutional guidelines.General consent was obtained according to the institutional guidelines.None of the authors have any conflicts of interests to declare. The authors received no pharmaceutical or industrial support for this study. No further direct or indirect financial support or other assets were transferred to the authors or their family members for this study. The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
LinkOut - more resources
Full Text Sources
Research Materials
