

Patterns and disparities of care in glioblastoma
- PMID: 30740232
- PMCID: PMC6352755
- DOI: 10.1093/nop/npy014
Patterns and disparities of care in glioblastoma
Abstract
Background: Glioblastoma is an aggressive disease with a defined standard of care offering crucial survival benefits. Disparities in care may influence treatment decisions. This study seeks to evaluate potential patterns in care delivery using the National Cancer Database (NCDB).
Methods: We evaluated the NCDB from 1998 to 2011 for patients diagnosed with glioblastoma older than 20 years of age in order to describe current hospital-based demographics, rates of treatment modality by age, race, gender, likelihood of receiving treatment, and survival probabilities.
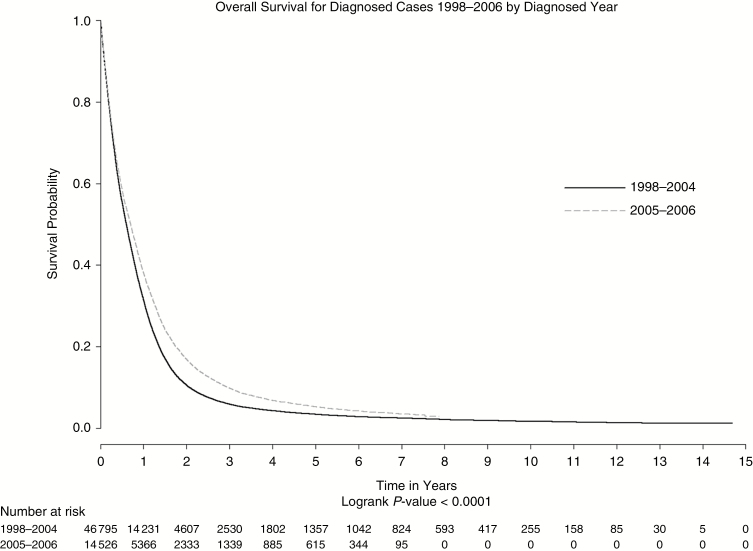
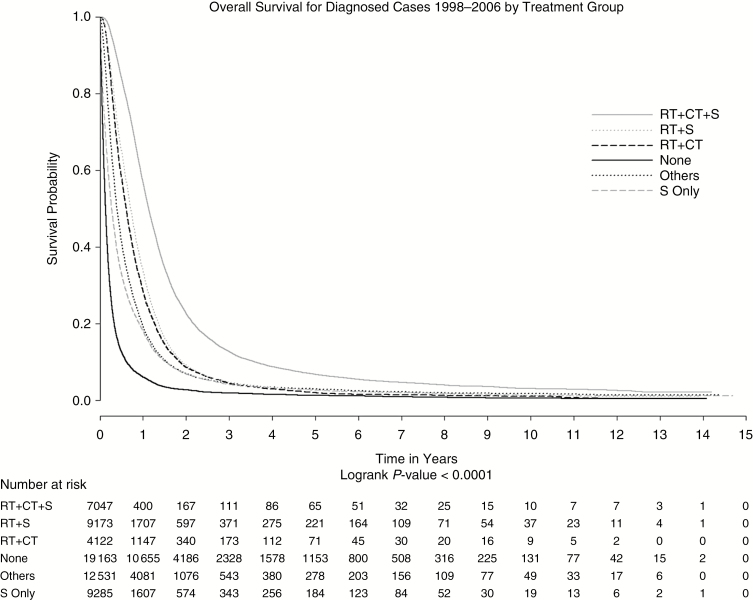
Results: From 1998 to 2011, 100672 patients were diagnosed with glioblastoma in the United States. Of these, 54% were younger than 65 years of age, while 20% were 75 years of age or older. The most common type of treatment was surgery (73%), followed by radiation (69%) and chemotherapy (50%). Eleven percent of patients did not receive any form of therapy. Patients receiving no form of treatment were more likely to be older, female, black, or Hispanic. Tumors that did not involve brainstem, ventricles, or the cerebellum were associated with more aggressive treatment and better overall survival. The median survival was 7.5 months. The use of concomitant surgical resection, chemotherapy, and radiation demonstrated greater survival benefit.
Conclusions: Median survival for glioblastoma is significantly less than reported in clinical trials. Sociodemographic factors such as age, gender, race, and socioeconomic status affect treatment decisions for glioblastoma. The elderly are greatly undertreated, as many elderly patients receive no treatment or significantly less than standard of care.
Keywords: Glioblastoma; patterns of care; survival; treatment.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Stupp R, Taillibert S, Kanner AA, et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: a randomized clinical trial. JAMA. 2015;314(23):2535–2543. - PubMed
