

Improving medical care and prevention in adults with congenital heart disease-reflections on a global problem-part II: infective endocarditis, pulmonary hypertension, pulmonary arterial hypertension and aortopathy
- PMID: 30740319
- PMCID: PMC6331381
- DOI: 10.21037/cdt.2018.10.16
Improving medical care and prevention in adults with congenital heart disease-reflections on a global problem-part II: infective endocarditis, pulmonary hypertension, pulmonary arterial hypertension and aortopathy
Abstract
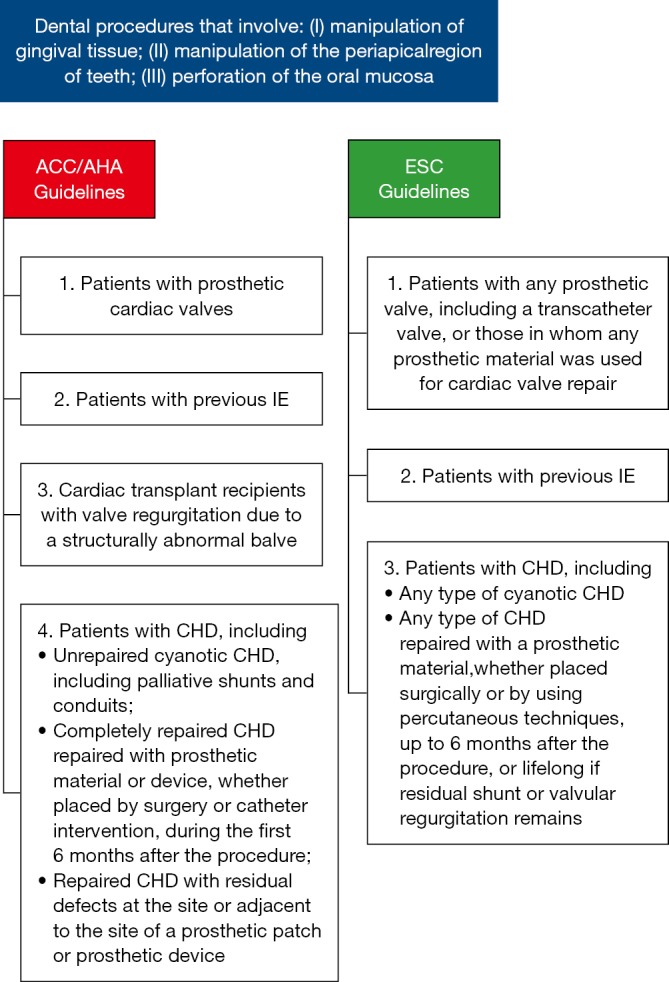
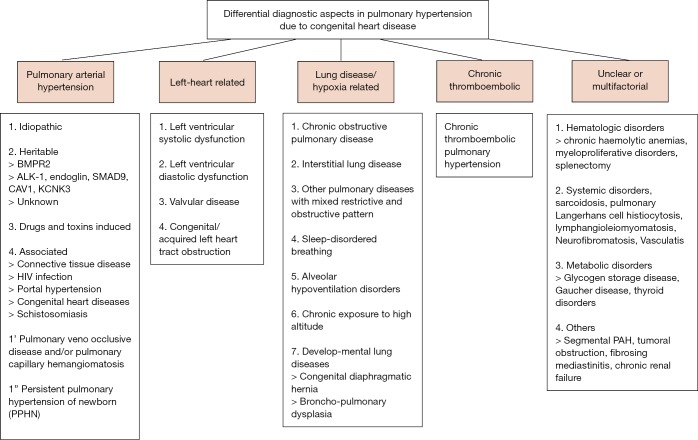
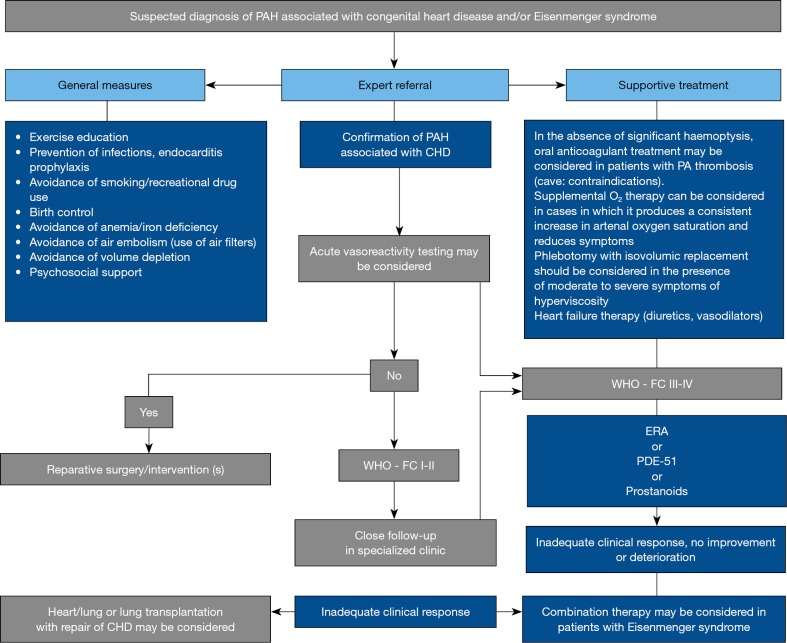
Despite relevant residua and sequels, follow-up care of adults with congenital heart disease (ACHD) is too often not performed by/in specialized and/or certified physicians or centers although major problems in the long-term course may develop. The most relevant encompass heart failure, cardiac arrhythmias, heart valve disorders, pulmonary vascular disease, infective endocarditis (IE), aortopathy and non-cardiac comorbidities. The present publication emphasizes current data on IE, pulmonary and pulmonary arterial hypertension and aortopathy in ACHD and underlines the deep need of an experienced follow-up care by specialized and/or certified physicians or centers, as treatment regimens from acquired heart disease can not be necessarily transmitted to CHD. Moreover, the need of primary and secondary medical prevention becomes increasingly important in order to reduce the burden of disease as well as the socioeconomic burden and costs in this particular patient group.
Keywords: Congenital heart defect (CHD); aortopathy; endocarditis; heart failure; prevention; primary health care; pulmonary hypertension.
Conflict of interest statement
Conflicts of Interest: R Neidenbach received research grants (“Unrestricted educational grant”) from Actelion Pharmaceuticals Deutschland GmbH and from the German Heart Foundation (“Deutsche Herzstiftung e.V.”) and the patient organization “Herzkind e. V.”; H Kaemmerer received fees and/or travel expenses for consulting activities and/or lectures from the following companies within the last 3 years: Actelion, Pfizer, Bayer-Healthcare, Bristol-Myers Squibb; D Pittrow has received speaker fees or honoraria for consultations from Actelion, Bayer, Genzyme, Boehringer Ingelheim, Novartis, MSD. and Dr. Erwin Oechslin currently holds the “Bitove Family Professorship for Adult Congenital Heart Disease”. Other author have no conflicts of interest to declare.
Figures
References
-
- Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 2015;132:1435-86. 10.1161/CIR.0000000000000296 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources