

Combined Heart and Kidney Transplantation: Clinical Experience in 100 Consecutive Patients
- PMID: 30741603
- PMCID: PMC6405671
- DOI: 10.1161/JAHA.118.010570
Combined Heart and Kidney Transplantation: Clinical Experience in 100 Consecutive Patients
Abstract
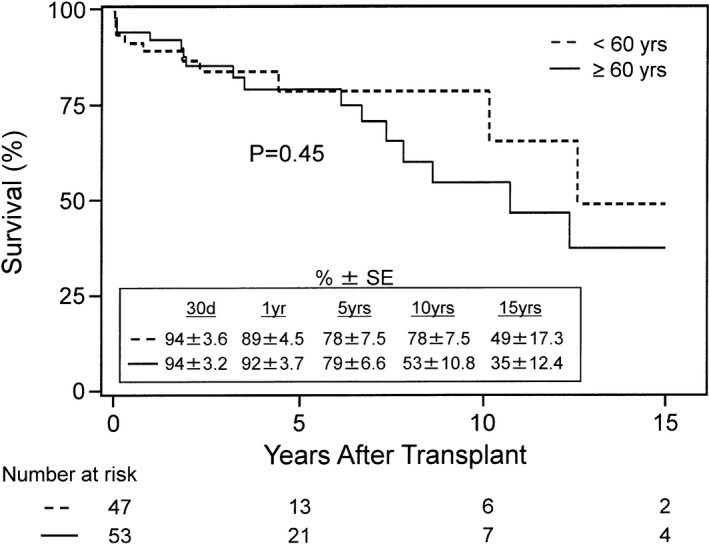
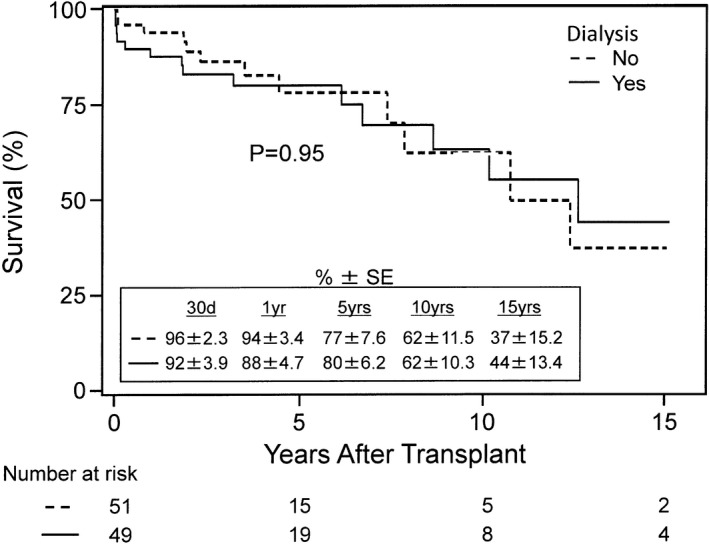
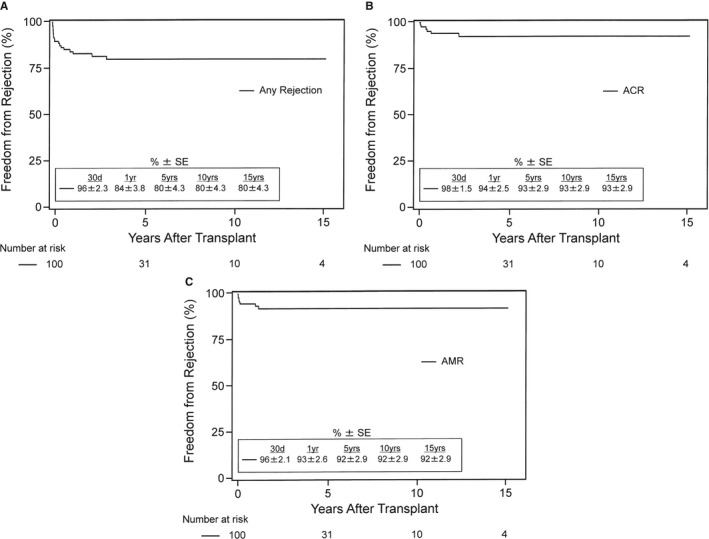
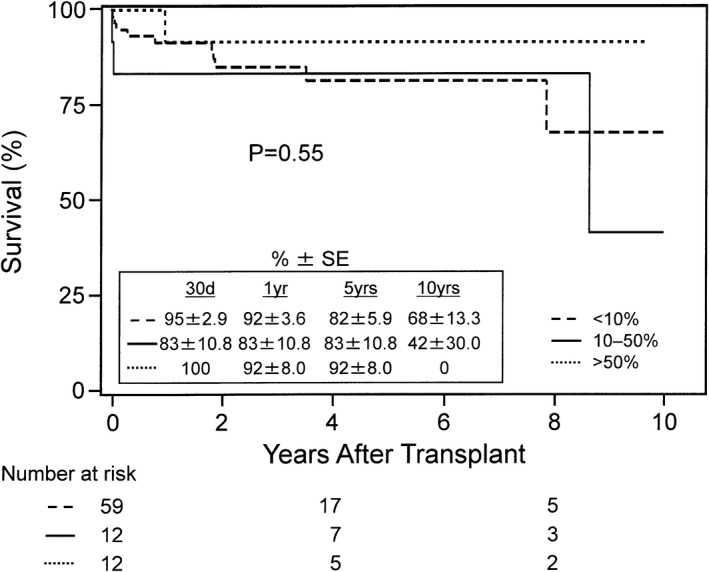
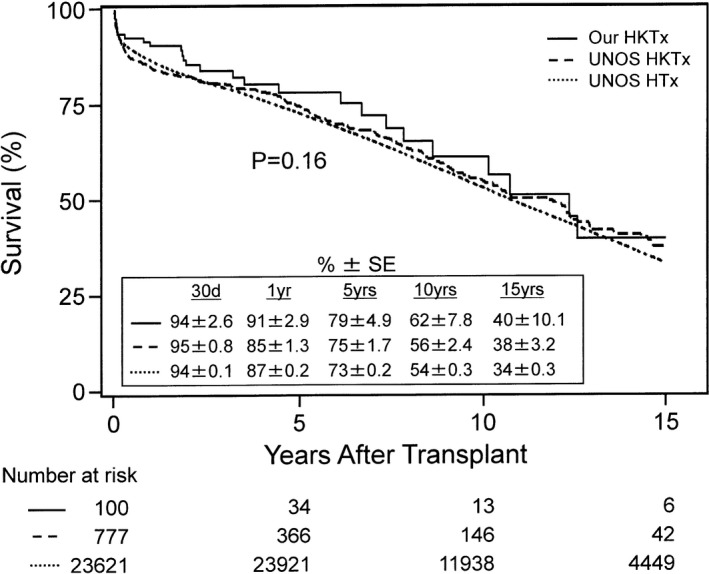
Background Combined heart and kidney transplantation ( HKT x) is performed in patients with severe heart failure and advanced renal insufficiency. We analyzed the long-term survival after HKT x, the influence of age and dialysis status, the rates of cardiac rejection, and the influence of sensitization. Methods and Results From June 1992 to December 2016, we performed 100 HKT x procedures. We compared older (≥60 years, n=53) with younger (<60 years, n=47) recipients, and recipients on preoperative dialysis (n=49) and not on dialysis (n=51). We analyzed actuarial freedom from any cardiac rejection, acute cellular rejection, and antibody-mediated rejection, and survival rates by sensitized status with panel-reactive antibody levels <10%, 10% to 50%, and >50%, and compared these survival rates with those from the United Network for Organ Sharing database. There was no difference in 15-year survival between the 2 age groups (35±12.4% and 49±17.3%, ≥60 versus <60 years; P=0.45). There was no difference in 15-year survival between the dialysis and nondialysis groups (44±13.4% and 37±15.2%, P=0.95). Actuarial freedom from any cardiac rejection ( acute cellular rejection >0 or antibody-mediated rejection >0) was 92±2.8% and 84±3.8%, acute cellular rejection (≥2R/3A) 98±1.5% and 94±2.5%, and antibody-mediated rejection (≥1) 96±2.1% and 93±2.6% at 30 days and 1 year after HKT x. There was no difference in the 5-year survival among recipients by sensitization status with panel-reactive antibody levels <10%, 10% to 50%, and >50% (82±5.9%, 83±10.8%, and 92±8.0%; P=0.55). There was no difference in 15-year survival after HKT x between the United Network for Organ Sharing database and our center (38±3.2% and 40±10.1%, respectively; P=0.45). Conclusions HKT x is safe to perform in patients 60 years and older or younger than 60 years and with or without dialysis dependence, with excellent outcomes. The degree of panel-reactive antibody sensitization did not appear to affect survival after HKT x.
Keywords: heart failure; heart transplantation; hemodialysis; kidney transplantation; mortality; renal disease.
Figures
References
-
- Lund LH, Khush KK, Cherikh WS, Goldfarb S, Kucheryavaya AY, Levvey BJ, Meiser B, Rossano JW, Chambers DC, Yusen RD, Stehlik J; International Society for Heart and Lung Transplantation . The Registry of the International Society for Heart and Lung Transplantation: Thirty‐Fourth Adult Heart Transplantation Report‐2017; Focus Theme: allograft ischemic time. J Heart Lung Transplant. 2017;36:1037–1046. - PubMed
-
- Schaffer JM, Chiu P, Singh SK, Oyer PE, Reitz BA, Mallidi HR. Heart and combined heart‐kidney transplantation in patients with concomitant renal insufficiency and end‐stage heart failure. Am J Transplant. 2014;14:384–396. - PubMed
-
- Gill J, Shah T, Hristea I, Chavalitdhamrong D, Anastasi B, Takemoto SK, Bunnapradist S. Outcomes of simultaneous heart‐kidney transplant in the US: a retrospective analysis using OPTN/UNOS data. Am J Transplant. 2009;9:844–852. - PubMed
-
- Habib PJ, Patel PC, Hodge D, Chimato N, Yip DS, Hosenpud JD, Wadei HM. Pre‐orthotopic heart transplant estimated glomerular filtration rate predicts post‐transplant mortality and renal outcomes: an analysis of the UNOS database. J Heart Lung Transplant. 2016;35:1471–1479. - PubMed
-
- Kolsrud O, Karason K, Holmberg E, Ricksten SE, Felldin M, Samuelsson O, Dellgren G. Renal function and outcome after heart transplantation. J Thorac Cardiovasc Surg. 2018;155:1593–1604. - PubMed
