

Inter-Rater Reliability of the Modified Radiographic Union Score for Diaphyseal Tibial Fractures With Bone Defects
- PMID: 30741726
- PMCID: PMC6534445
- DOI: 10.1097/BOT.0000000000001445
Inter-Rater Reliability of the Modified Radiographic Union Score for Diaphyseal Tibial Fractures With Bone Defects
Abstract
Objectives: To evaluate inter-rater reliability of the modified Radiographic Union Score for Tibial (mRUST) fractures among patients with open, diaphyseal tibia fractures with a bone defect treated with intramedullary nails (IMNs), plates, or definitive external fixation (ex-fix).
Design: Retrospective cohort study.
Setting: Fifteen-level one civilian trauma centers; 2 military treatment facilities.
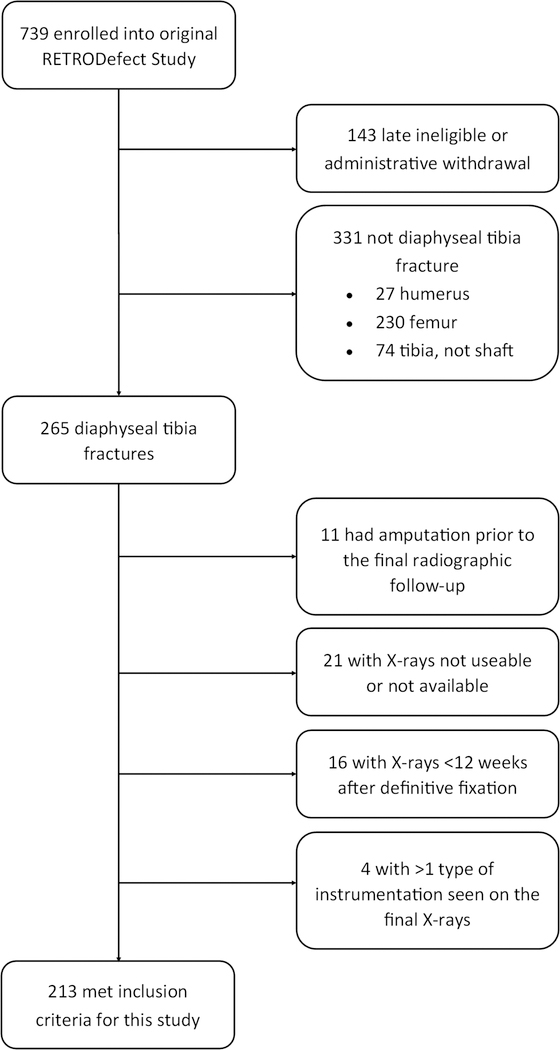
Patients/participants: Patients ≥18 years old with open, diaphyseal tibia fractures with a bone defect ≥1 cm surgically treated between 2007 and 2012.
Intervention: Three of 6 orthopedic traumatologists reviewed and applied mRUST scoring criteria to radiographs from the last clinical visit within 13 months of injury.
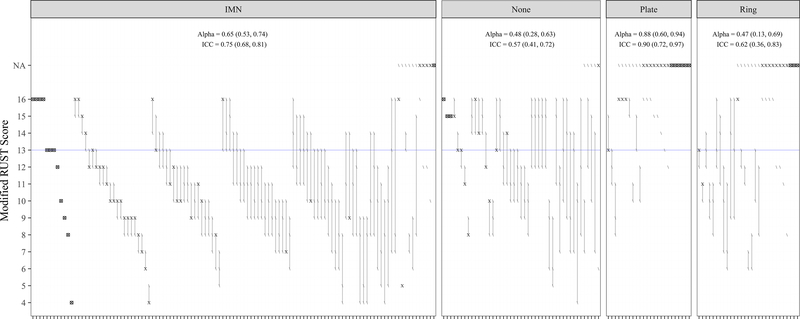
Main outcome measurements: Inter-rater reliability was assessed using Krippendorff's alpha (KA) statistic; intraclass correlation coefficient (ICC) is presented for comparison with previous publications.
Results: Two hundred thirteen patients met inclusion criteria including 115 IMNs, 24 plates, 29 ex-fixes, and 45 cases that no longer had instrumentation at evaluation. All reviewers agreed on the pattern of scoreable cortices for 90.4% of IMNs, 88.9% of those without instrumentation, 44.8% of rings, and 20.8% of plates. Thirty-one (15%) cases, primarily plates and ex-fixes, did not contribute to KA and ICC estimates because <2 raters scored all cortices. The overall KA for the 85% that could be analyzed was 0.64 (ICC 0.71). For IMNs, plates, ex-fixes, and no instrumentation, KA (ICC) was 0.65 (0.75), 0.88 (0.90), 0.47 (0.62), and 0.48 (0.57), respectively.
Conclusions: In tibia fractures with bone defects, the mRUST seems similarly reliable to previous work in patients treated with IMN but is less reliable in those with plates or ex-fixes, or after removal of instrumentation.
Conflict of interest statement
Figures

References
-
- Bhandari M, Guyatt GH, Swiontkowski MF, Tornetta P, Sprague S, Schemitsch EH. A lack of consensus in the assessment of fracture healing among orthopaedic surgeons. J Orthop Trauma. 2002;16(8):562–566. Accessed Nov 21, 2017. - PubMed
-
- Whelan DB, Bhandari M, Stephen D, et al. Development of the radiographic union score for tibial fractures for the assessment of tibial fracture healing after intramedullary fixation. J Trauma. 2010;68(3):629–632. https://www.ncbi.nlm.nih.gov/pubmed/19996801. Accessed Nov 21, 2017. doi: 10.1097/TA.0b013e3181a7c16d. - DOI - PubMed
