

Esophagogastric Junction Distensibility on Functional Lumen Imaging Probe Topography Predicts Treatment Response in Achalasia-Anatomy Matters!
- PMID: 30741739
- PMCID: PMC6682473
- DOI: 10.14309/ajg.0000000000000137
Esophagogastric Junction Distensibility on Functional Lumen Imaging Probe Topography Predicts Treatment Response in Achalasia-Anatomy Matters!
Abstract
Introduction: To compare the utility of the distensibility index (DI) on functional lumen imaging probe (FLIP) topography to other esophagogastric junction (EGJ) metrics in assessing treatment response in achalasia in the context of esophageal anatomy.
Methods: We prospectively evaluated 79 patients (at ages 17-81 years; 47% female patients) with achalasia during follow-up after pneumatic dilation, Heller myotomy, or per-oral endoscopic myotomy with timed barium esophagram, high-resolution impedance manometry, and FLIP. Anatomic deformities were identified based on consensus expert opinion. Patients were classified based on anatomy and EGJ opening to determine the association with radiographic outcome and Eckardt score (ES).
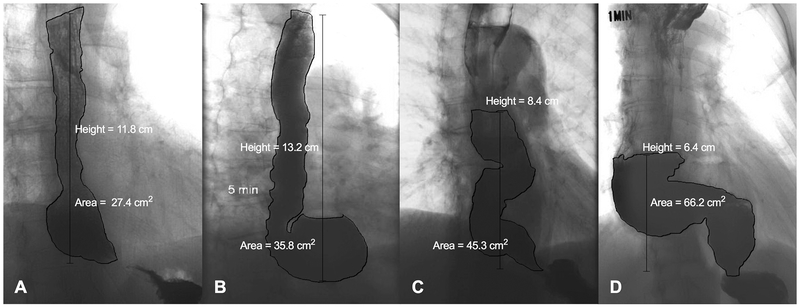
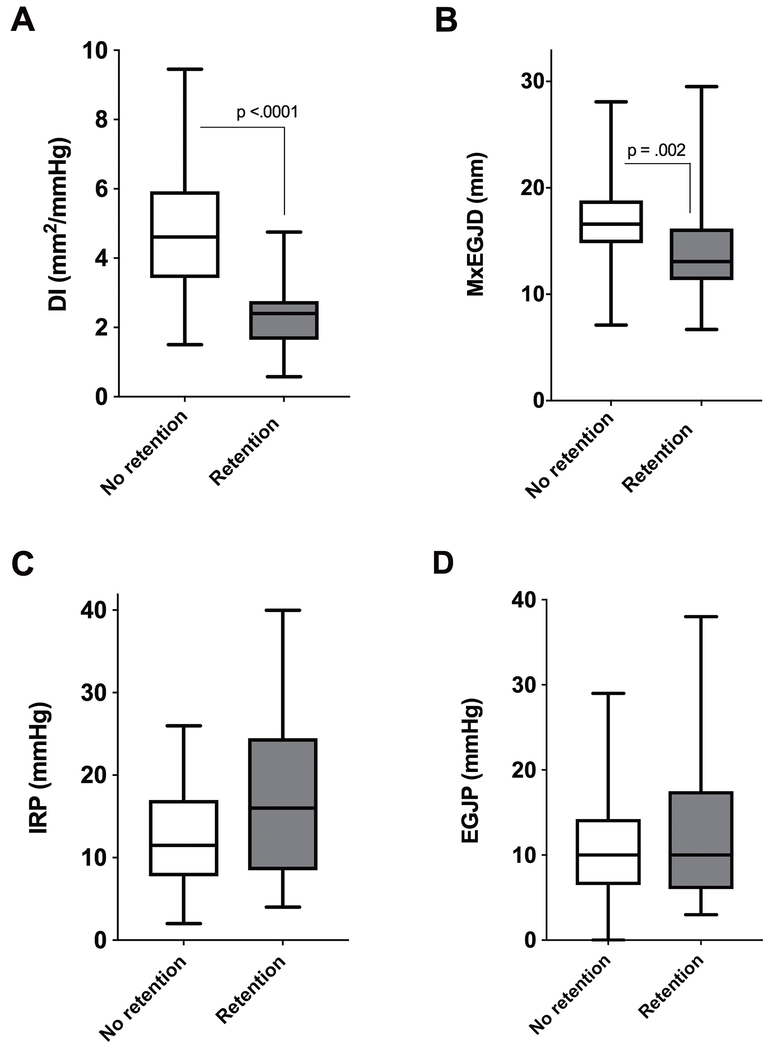
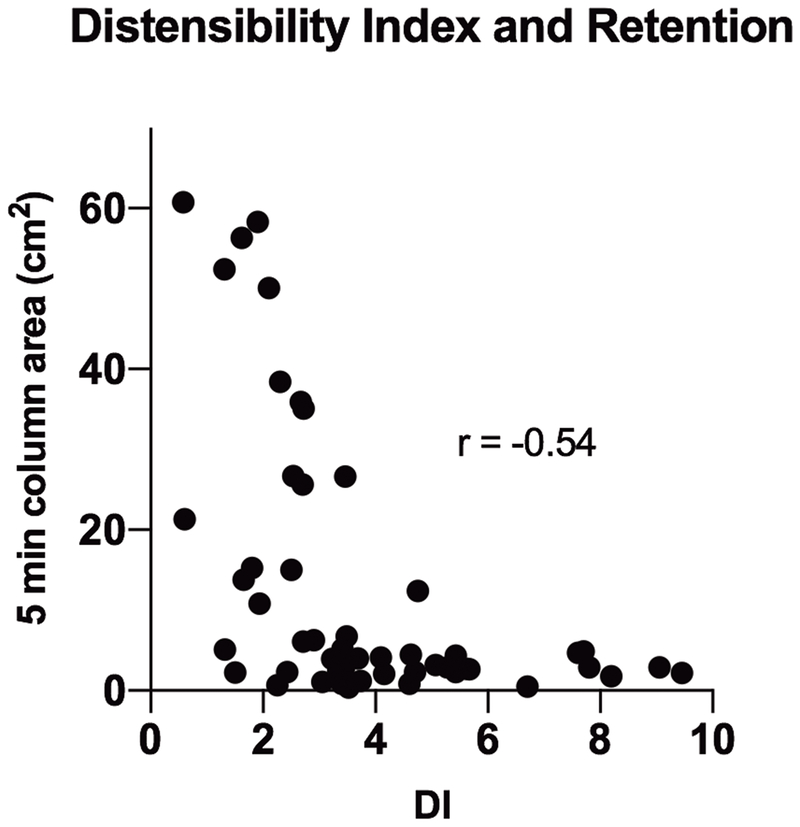
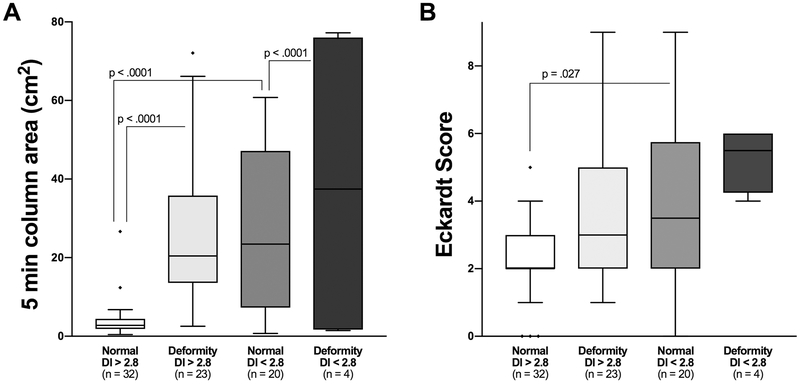
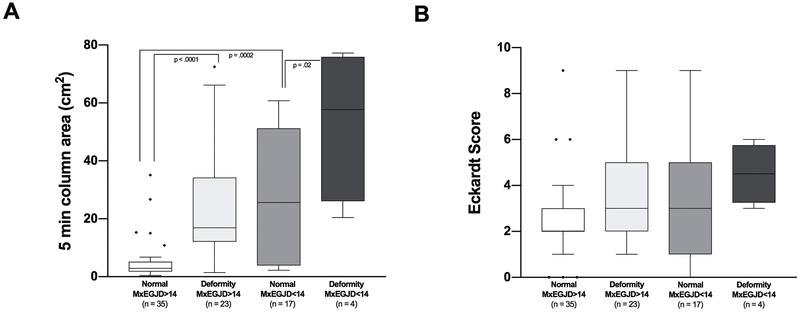
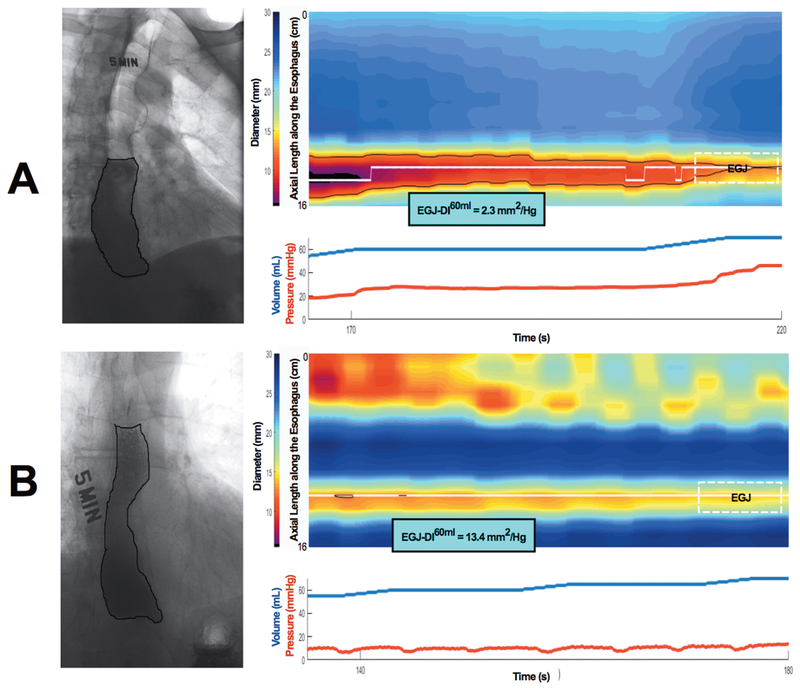
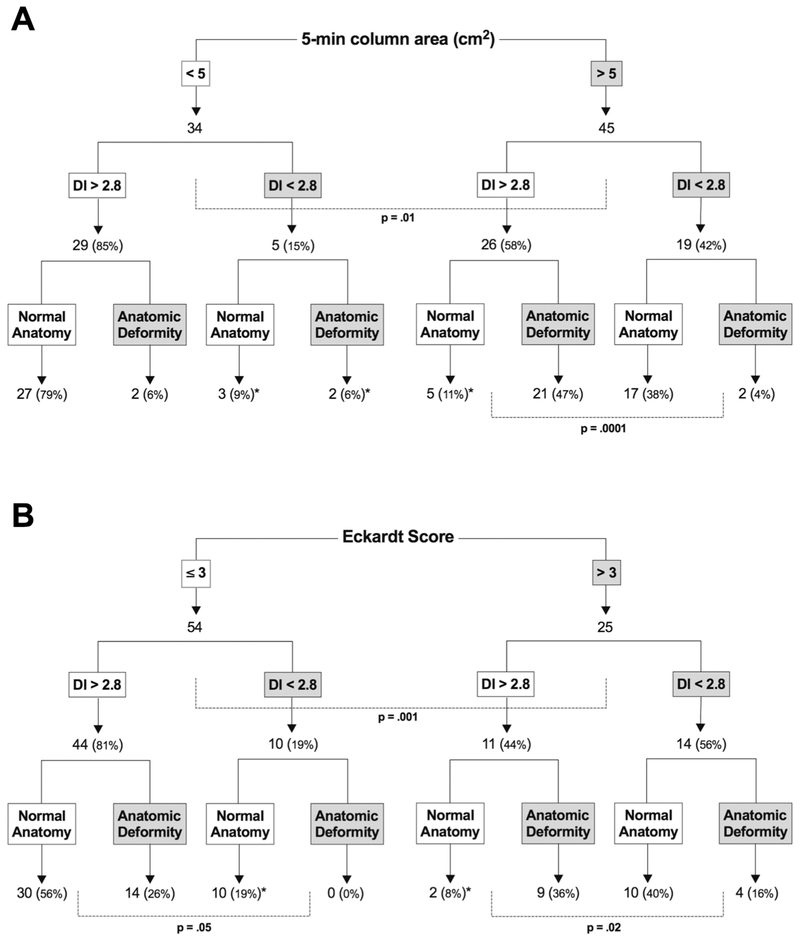
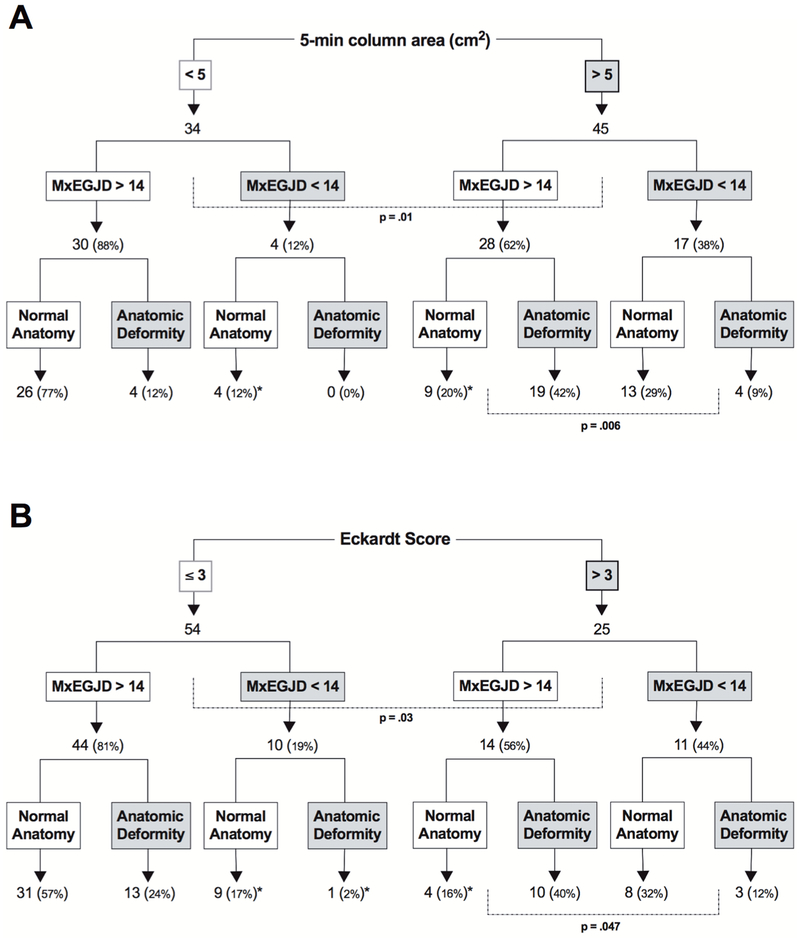
Results: Twenty-seven patients (34.1%) had an anatomic deformity-10 pseudodiverticula at myotomy, 7 epiphrenic diverticula, 5 sigmoid, and 5 sinktrap. A 5-minute column area of >5 cm was best associated with an ES of >3, with a sensitivity of 84% (P = 0.0013). Area under the curve for EGJ metrics in association with retention was as follows: DI, 0.90; maximal EGJ diameter, 0.76; integrated relaxation pressure, 0.64; and basal esophagogastric junction pressure, 0.53. Only FLIP metrics were associated with retention given normal anatomy (DI 2.4 vs 5.2 mm/mm Hg and maximal EGJ diameter 13.1 vs 16.6 mm in patients with and without retention, respectively; P values < 0.0001 and 0.002). Using a DI cutoff of <2.8 as abnormal, 40 of 45 patients with retention (P = 0.0001) and 23 of 25 patients with an ES of >3 (P = 0.02) had a low DI and/or anatomic deformity. With normal anatomy, 21 of 22 patients with retention had a low or borderline low DI.
Discussion: The FLIP DI is most useful metric for assessing the effect of achalasia treatment on EGJ opening. However, abnormal anatomy is an important mediator of outcome and treatment success will be modulated by anatomic defects that impede bolus emptying.
Conflict of interest statement
CONFLICTS OF INTEREST / STUDY SUPPORT
Potential competing interests:
Dustin Carlson, Peter Kahrilas, and John Pandolfino have intellectual property rights surrounding endoFLIP technology
Figures
References
-
- Saleh CM, Ponds FA, Schijven MP, et al. Efficacy of pneumodilation in achalasia after failed Heller myotomy. Neurogastroenterol Motil 2016;28:1741–1746. - PubMed
-
- Salvador R, Voltarel G, Savarino E, et al. The natural history of achalasia: Evidence of a continuum-”The evolutive pattern theory”. Dig Liver Dis 2017. - PubMed
-
- Rohof WO, Salvador R, Annese V, et al. Outcomes of treatment for achalasia depend on manometric subtype. Gastroenterology 2013;144:718–25; quiz e13–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
