

Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma
- PMID: 30742122
- PMCID: PMC6408961
- DOI: 10.1038/s41591-018-0337-7
Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma
Abstract
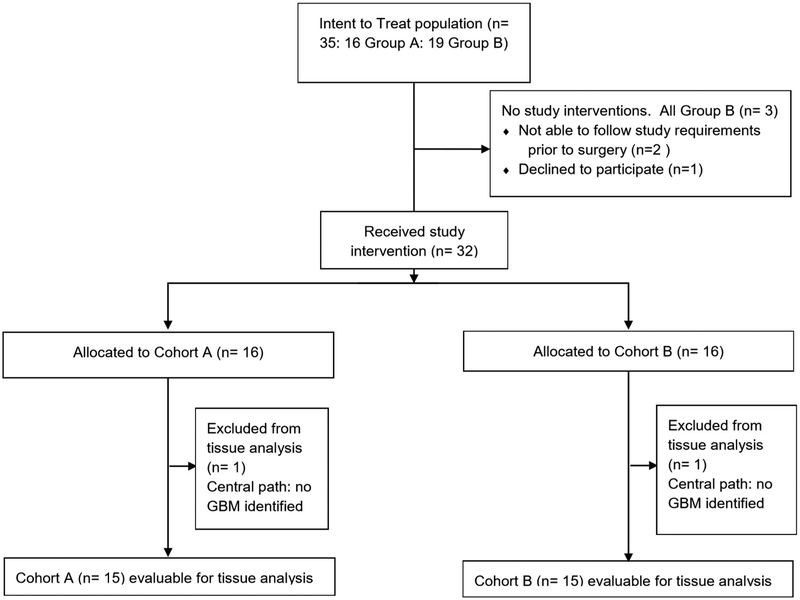
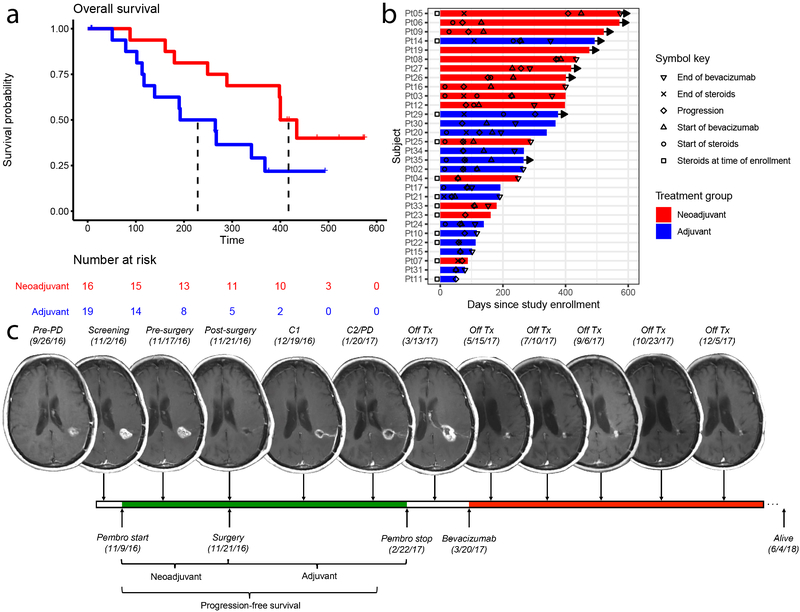
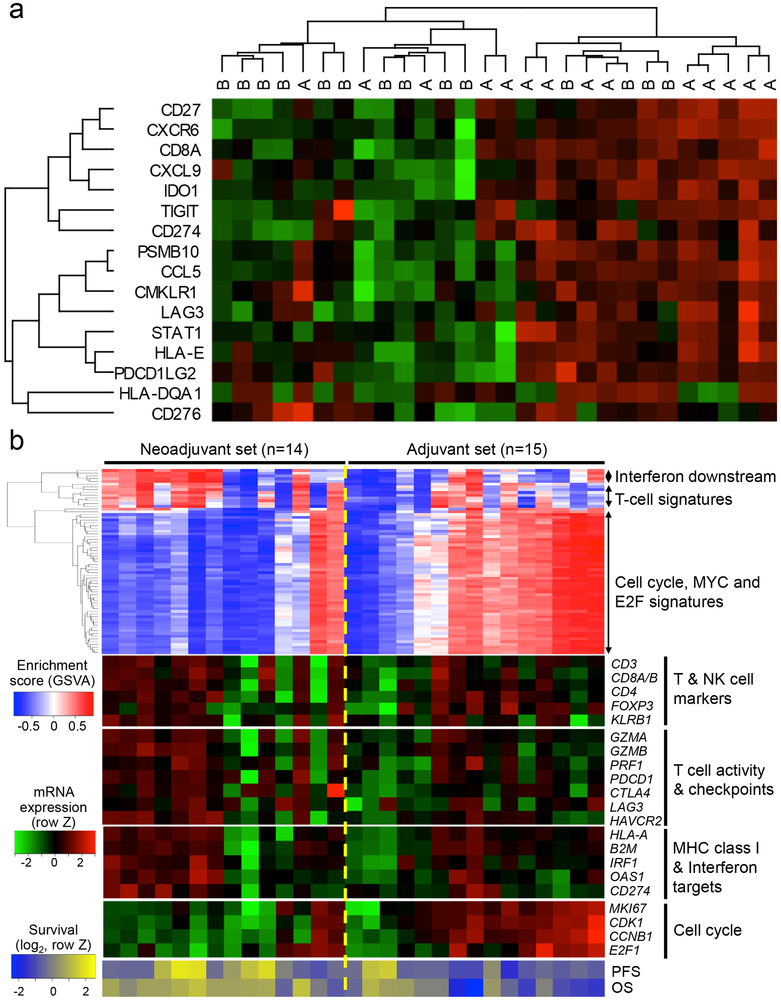
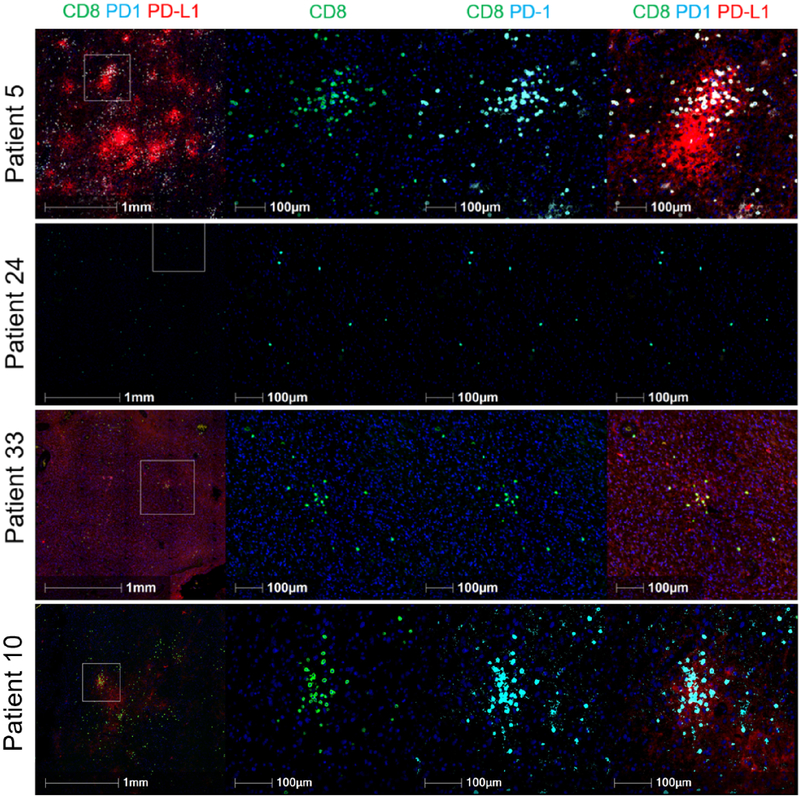
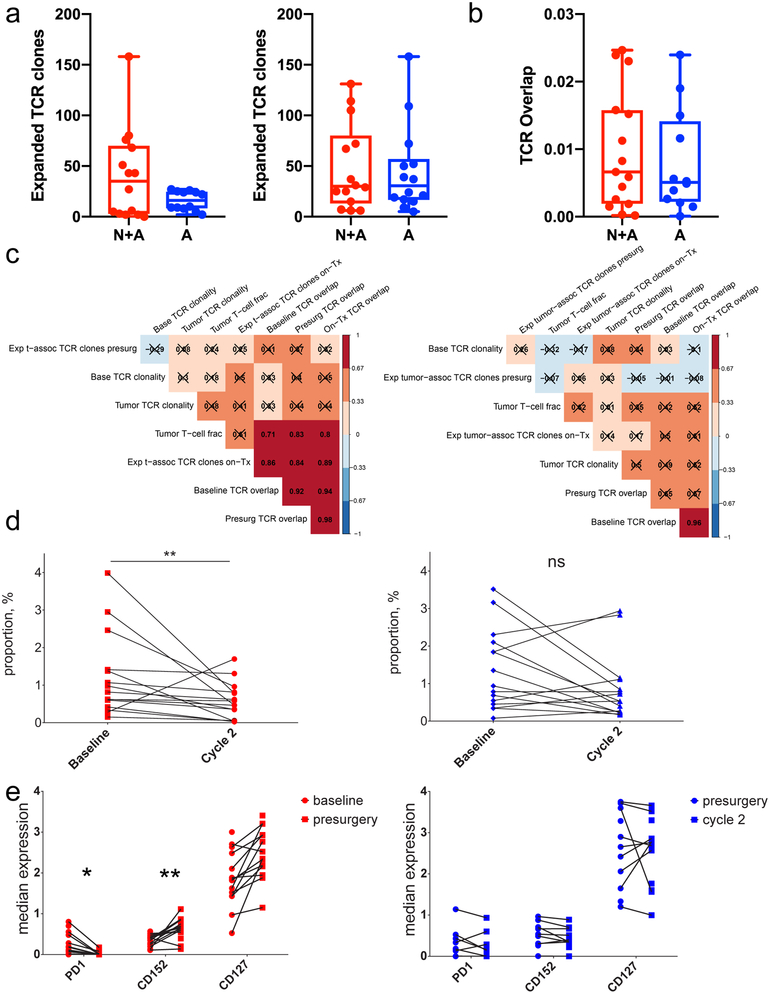
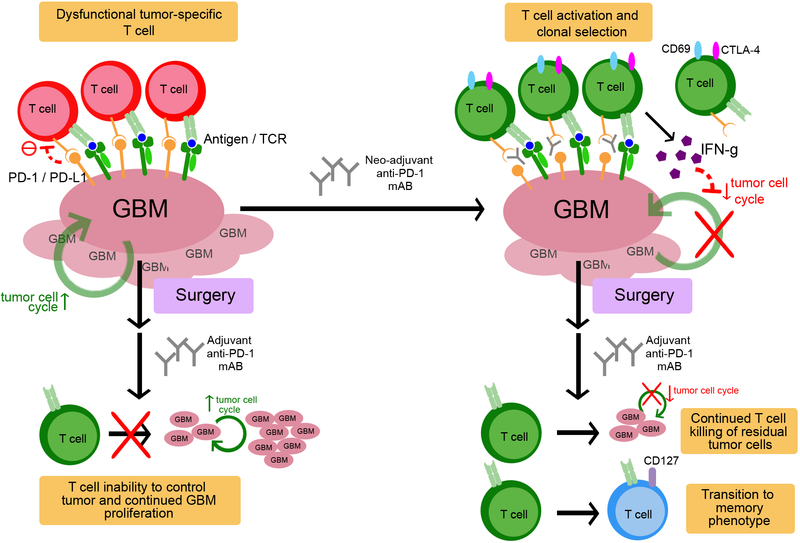
Glioblastoma is the most common primary malignant brain tumor in adults and is associated with poor survival. The Ivy Foundation Early Phase Clinical Trials Consortium conducted a randomized, multi-institution clinical trial to evaluate immune responses and survival following neoadjuvant and/or adjuvant therapy with pembrolizumab in 35 patients with recurrent, surgically resectable glioblastoma. Patients who were randomized to receive neoadjuvant pembrolizumab, with continued adjuvant therapy following surgery, had significantly extended overall survival compared to patients that were randomized to receive adjuvant, post-surgical programmed cell death protein 1 (PD-1) blockade alone. Neoadjuvant PD-1 blockade was associated with upregulation of T cell- and interferon-γ-related gene expression, but downregulation of cell-cycle-related gene expression within the tumor, which was not seen in patients that received adjuvant therapy alone. Focal induction of programmed death-ligand 1 in the tumor microenvironment, enhanced clonal expansion of T cells, decreased PD-1 expression on peripheral blood T cells and a decreasing monocytic population was observed more frequently in the neoadjuvant group than in patients treated only in the adjuvant setting. These findings suggest that the neoadjuvant administration of PD-1 blockade enhances both the local and systemic antitumor immune response and may represent a more efficacious approach to the treatment of this uniformly lethal brain tumor.
Figures





Comment in
-
Molecular responses to immune checkpoint blockade in glioblastoma.Nat Med. 2019 Mar;25(3):359-361. doi: 10.1038/s41591-019-0385-7. Nat Med. 2019. PMID: 30842671 Free PMC article.
-
Neoadjuvant anti-PD-1 immunotherapy for recurrent glioblastoma.Transl Cancer Res. 2019 Dec;8(Suppl 6):S577-S579. doi: 10.21037/tcr.2019.05.24. Transl Cancer Res. 2019. PMID: 32864354 Free PMC article. No abstract available.
References
-
- Stupp R, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352, 987–996 (2005). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
