

Delayed Antibiotic Therapy and Organ Dysfunction in Critically Ill Septic Patients in the Emergency Department
- PMID: 30744073
- PMCID: PMC6406307
- DOI: 10.3390/jcm8020222
Delayed Antibiotic Therapy and Organ Dysfunction in Critically Ill Septic Patients in the Emergency Department
Abstract
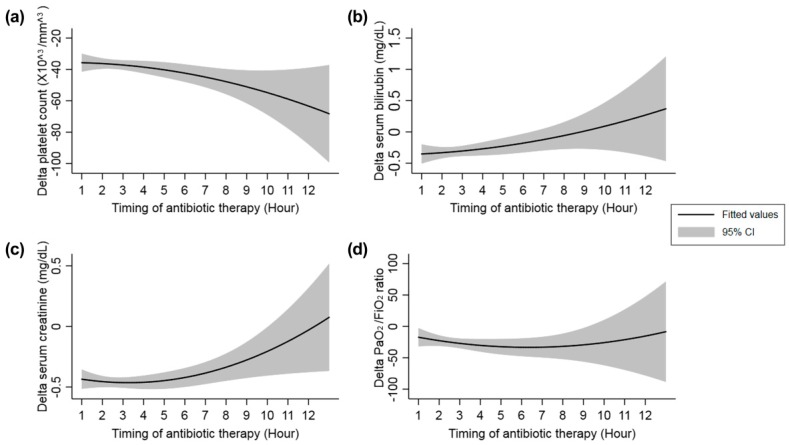
Background: We investigated the effect of antibiotic timing on outcomes based on changes in surrogate markers of organ failure, including platelet, serum bilirubin, serum creatinine levels, and the PaO₂/FiO₂ (P/F) ratio.
Methods: This was a single-center, retrospective observational study of critically ill septic patients who presented to the emergency department (ED). The study period extended from August 2008 to September 2016. The primary outcomes included changes in platelet, serum bilirubin, serum creatinine levels, and the P/F ratio (δ-platelet, δ-serum bilirubin, δ-serum creatinine, and δ-P/F ratio were calculated as values measured on Day 3; values measured at ED enrollment). A multivariable linear regression model was developed to assess variables related to outcomes (δ-platelet, δ-serum bilirubin, δ-serum creatinine, and δ-P/F ratio).
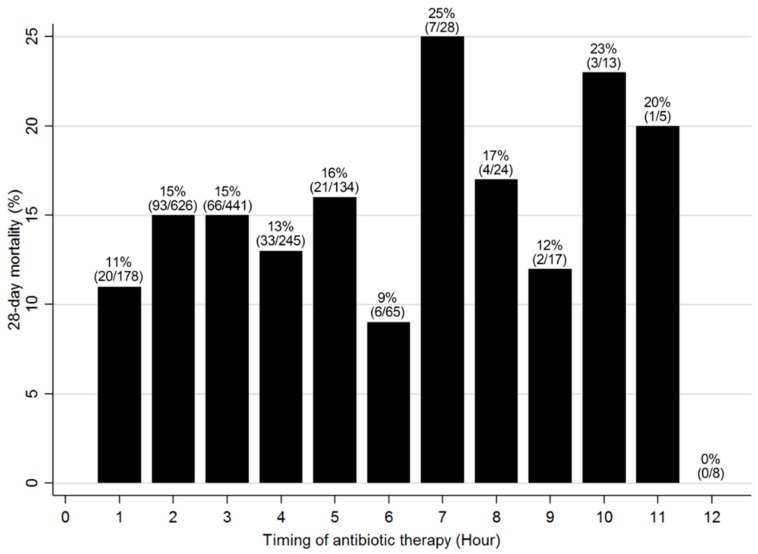
Results: We analyzed 1784 patients who met the inclusion criteria. The overall 28-day mortality was 14% (n = 256/1784). On multivariable linear regression analysis, the hourly delay in antibiotic therapy was significantly associated with a decrease in δ-platelet count (coefficient, -1.741; standard error, 0.740; p = 0.019), and an increase in δ-serum bilirubin (coefficient, 0.054; standard error, 0.021; p = 0.009). In contrast, it was not associated with δ-creatinine (coefficient, 0.008; standard error, 0.010; p = 0.434) or the δ-P/F ratio (coefficient, -0.797; standard error, 1.858; p = 0.668).
Conclusion: The hourly delay of antibiotic therapy was associated with decreased platelet count and increased serum bilirubin concentration in critically ill septic patients during the first three days of ED admission.
Keywords: antibacterial agents; multiple organ failure; sepsis; septic shock; timing.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Singer M., Deutschman C.S., Seymour C.W., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.D., Coopersmith C.M., et al. The third international consensus definitions for sepsis and septic shock (sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Seymour C.W., Liu V.X., Iwashyna T.J., Brunkhorst F.M., Rea T.D., Scherag A., Rubenfeld G., Kahn J.M., Shankar-Hari M., Singer M., et al. Assessment of clinical criteria for sepsis: For the third international consensus definitions for sepsis and septic shock (sepsis-3) JAMA. 2016;315:762–774. doi: 10.1001/jama.2016.0288. - DOI - PMC - PubMed
-
- Rhodes A., Evans L.E., Alhazzani W., Levy M.M., Antonelli M., Ferrer R., Kumar A., Sevransky J.E., Sprung C.L., Nunnally M.E., et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Crit. Care Med. 2017;45:486–552. doi: 10.1097/CCM.0000000000002255. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
