

Facility delivery and postnatal care services use among mothers who attended four or more antenatal care visits in Ethiopia: further analysis of the 2016 demographic and health survey
- PMID: 30744583
- PMCID: PMC6371418
- DOI: 10.1186/s12884-019-2216-8
Facility delivery and postnatal care services use among mothers who attended four or more antenatal care visits in Ethiopia: further analysis of the 2016 demographic and health survey
Abstract
Background: Antenatal care provides the best opportunity to promote maternal and child health services use. But many Ethiopian mothers deliver at home and fail to attend postnatal care. Therefore, this study was done to identify factors associated with health facility delivery among mothers who attended four or more antenatal care visits. The study was also intended to identify factors associated with postnatal care service use among mothers who delivered at home after four or more antenatal care visits.
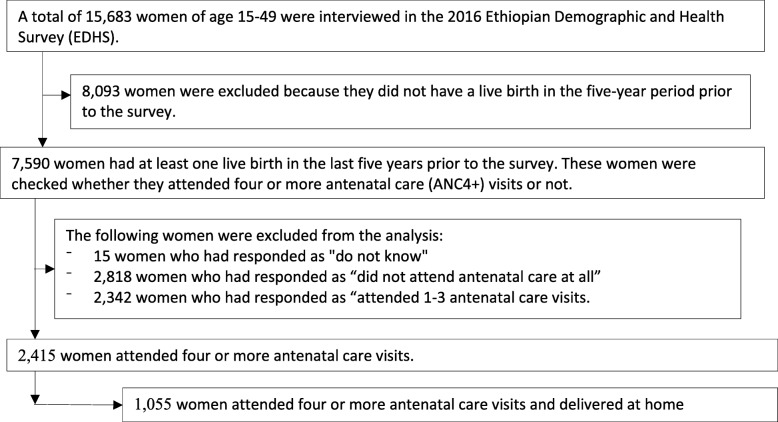
Methods: This study used the 2016 Ethiopian Demographic and Health Survey data. Two thousand four hundred fifteen women who attended four or more antenatal care visits were included to identify factors associated with health facility delivery after four or more antenatal care visits. Among them, 1055 mothers delivered at home. These women were included to identify factors associated with postnatal care service use. Stata 15.1 was used to analyze the data. Multivariable logistic regression model was fitted to identify associations between the outcome and predictor variables.
Results: Among women who had four or more antenatal care visits, 56% delivered at health facility. Mothers with secondary or higher level of education (AOR = 2.9; 95% CI = 1.6-5.3), urban residents (AOR = 3.4; 95% CI = 1.9-6.1), women with highest wealth quintile (AOR = 2.7; 95% CI = 1.5-4.8), and working women (AOR = 1.6; 95% CI = 1.2-2.3) had higher odds of delivering at health facilities. High birth order (AOR = 0.5; 95% CI = 0.3-0.7) was negatively associated with a lower likelihood of health facility delivery. Among women who delivered at home, only 8% received postnatal care within 42 days after delivery. Only the content of care received during antenatal care visits (AOR = 1.40; 95% CI = 1.1-1.8) was significantly associated with postnatal care attendance.
Conclusion: Women with lower socio-economic status had lower odds of giving birth at health facility even after attending antenatal care. The more antenatal care components a mother received, the higher her probability of delivering at health facility. Similarly, postnatal care attendance was higher among women who had received more antenatal care components.
Keywords: Antenatal care; Ethiopia; Facility delivery; Postnatal care; Quality of care.
Conflict of interest statement
Authors’ information
GAF is assistant professor in reproductive health in Bahir Dar University and PhD fellow in Pan African University, Institute of life (including Health and agriculture) and earth Sciences, University of Ibadan. FA is associate professor of public health in Bahir Dar University and a post-doctoral fellow of African Mental Health Research Initiative (AMARI) at Addis Ababa University. He earned his PhD in mental health epidemiology. SAK is also assistant professor of social works in Bahir Dar University. She earned her PhD in social work and development from Addis Ababa University and currently head of the department.
Ethics approval and consent to participate
The Ethiopian Demographic and health survey obtained written informed consent from all the participants during the data collection. Data were collected anonymously. The survey secured ethical clearance from the Ethiopian national Ethics review committee. Permission was obtained to analyze this data from the DHS program.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO, UNICEF, UNFPA, World Bank Group, The United Nations Population Division. Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division 2015.
-
- Black RE, Levin C, Walker N, Chou D, Liu L Temmerman M. Reproductive, maternal, newborn, and child health: key messages from disease control priorities 3rd edn. Lancet 2016;388(10061):2811–2824. - PubMed
-
- You DH, Ejdemyr L, Idele S, Hogan P, Mathers D, Gerland C, New P, Rou J, Leontine A. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN inter-agency group for child mortality estimation. Lancet. 2015;386(10010):2275–2286. doi: 10.1016/S0140-6736(15)00120-8. - DOI - PubMed
-
- WHO. Strategies towards ending preventable maternal mortality (EPMM). 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
