

Efficacy of a blended low-intensity internet-delivered psychological programme in patients with multimorbidity in primary care: study protocol for a randomized controlled trial
- PMID: 30744610
- PMCID: PMC6371446
- DOI: 10.1186/s12888-019-2037-3
Efficacy of a blended low-intensity internet-delivered psychological programme in patients with multimorbidity in primary care: study protocol for a randomized controlled trial
Abstract
Background: The World Health Organization (WHO) has included comorbidity between depression and a chronic disease among the 10 leading global health priorities. Although there is a high prevalence of multimorbidity, health care systems are mainly designed for the management of individual diseases. Given the difficulty in delivering face-to-face psychological treatments, alternative models of treatment delivery have been proposed, emphasizing the role of technologies such as the Internet. The aim of this study is to assess the efficacy in Primary Care (PC) of a blended low-intensity psychological intervention applied using information and communication technologies (ICTs) for the treatment of multimorbidity in PC (depression and type 2 diabetes/low back pain) by means of a randomized controlled trial (RCT). Our main hypothesis is that improved usual care combined with psychological therapy applied using ICTs will be more efficacious for improvement in the symptomatology of multimorbidity, compared to a group with only improved treatment as usual six months after the end of treatment.
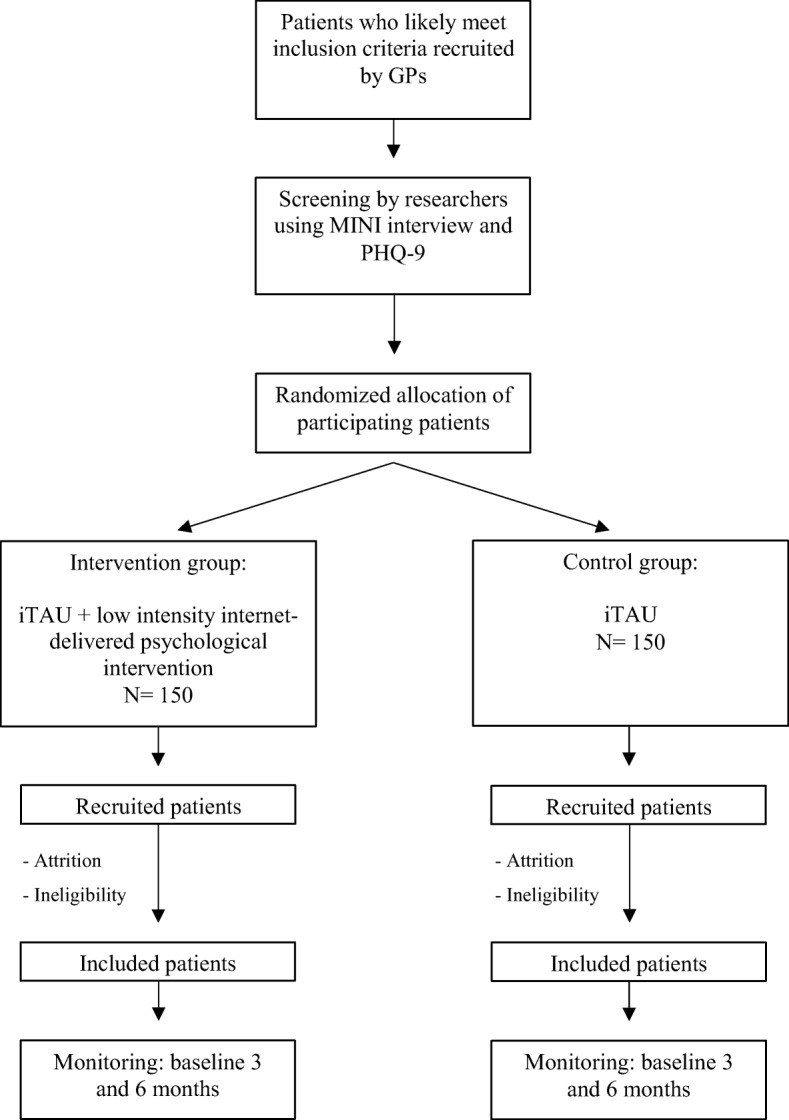
Methods: A protocol has been designed combining a face-to-face intervention with a supporting online programme that will be tested by an RCT conducted in three different regions (Andalusia, Aragon and the Balearic Islands). The RCT will evaluate three hundred participants diagnosed with depression and type 2 diabetes/low back pain. Four highly experienced research groups specializing in clinical psychology are involved in this trial, and there will be ample possibilities for translation and transfer to usual clinical practice.
Discussion: This clinical trial will lead to improvement in financial sustainability, maximizing the use of resources and responding to principles of efficiency and effectiveness. Furthermore, based on the evaluation of the feasibility of implementing this intervention in primary care facilities, we expect to be able to suggest the intervention for incorporation into public policy. In conclusion, positive results of this study could have a significant impact on one of the most important health-related problems, multimorbidity.
Trial registration: ClinicalTrials.gov, NCT03426709 . Registered retrospectively on 08 February 2018.
Keywords: Depression; Information and communication technologies (ICTs); Multimorbidity; Primary care; Randomized controlled trial (RCT).
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
This study is approved by the Research Ethics Committee of each autonomous community: (CEICA Aragon, CEIC Balearic Islands, and the Regional Ethics and Research Committee of the province of Malaga) and it is designed in accordance with the ethical standards laid down in the Declaration of Helsinki and its later amendments. Written informed consent will be obtained before screening and application of exclusion criteria takes place.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Smith SM, Soubhi H, Fortin M, Hudon C, O'Dowd T. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. 2012;4:CD006560. - PubMed
-
- Forjaz MJ, Rodriguez-Blazquez C, Ayala A, Rodriguez-Rodriguez V, de Pedro-Cuesta J, Garcia-Gutierrez S, Prados-Torres A. Chronic conditions, disability, and quality of life in older adults with multimorbidity in Spain. Eur J Intern Med. 2015;26(3):176–181. doi: 10.1016/j.ejim.2015.02.016. - DOI - PubMed
