

Persistent mutant oncogene specific T cells in two patients benefitting from anti-PD-1
- PMID: 30744692
- PMCID: PMC6371497
- DOI: 10.1186/s40425-018-0492-x
Persistent mutant oncogene specific T cells in two patients benefitting from anti-PD-1
Erratum in
-
Correction to: persistent mutant oncogene specific T cells in two patients benefitting from anti-PD-1.J Immunother Cancer. 2019 Mar 6;7(1):63. doi: 10.1186/s40425-019-0547-7. J Immunother Cancer. 2019. PMID: 30841906 Free PMC article.
Abstract
Background: Several predictive biomarkers are currently approved or are under investigation for the selection of patients for checkpoint blockade. Tumor PD-L1 expression is used for stratification of non-small cell lung (NSCLC) patients, with tumor mutational burden (TMB) also being explored with promising results, and mismatch-repair deficiency is approved for tumor site-agnostic disease. While tumors with high PD-L1 expression, high TMB, or mismatch repair deficiency respond well to checkpoint blockade, tumors with lower PD-L1 expression, lower mutational burdens, or mismatch repair proficiency respond much less frequently.
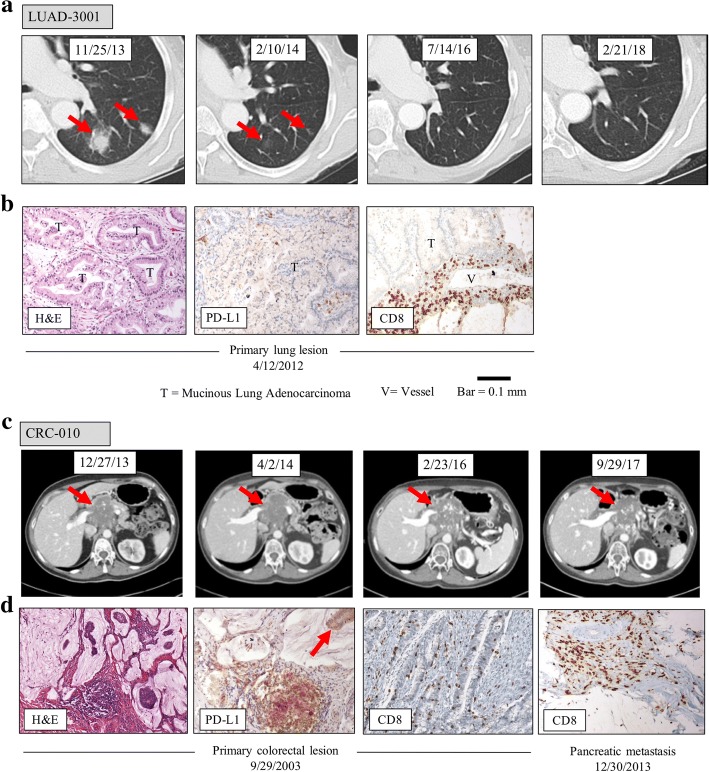
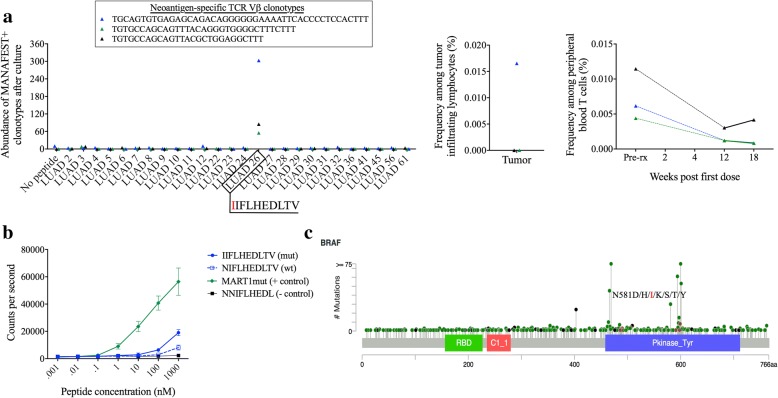
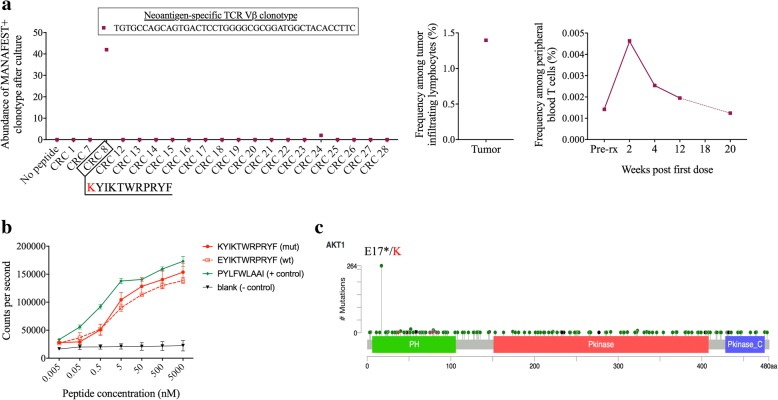
Case presentation: We studied two patients with unexpected responses to checkpoint blockade monotherapy: a patient with PD-L1-negative and low mutational burden NSCLC and one with mismatch repair proficient colorectal cancer (CRC), both of whom lack the biomarkers associated with response to checkpoint blockade, yet achieved durable clinical benefit. Both maintained T-cell responses in peripheral blood to oncogenic driver mutations - BRAF-N581I in the NSCLC and AKT1-E17K in the CRC - years after treatment initiation. Mutation-specific T cells were also found in the primary tumor and underwent dynamic perturbations in the periphery upon treatment.
Conclusions: These findings suggest that T cell responses to oncogenic driver mutations may be more prevalent than previously appreciated and could be harnessed in immunotherapeutic treatment, particularly for patients who lack the traditional biomarkers associated with response. Comprehensive studies are warranted to further delineate additional predictive biomarkers and populations of patients who may benefit from checkpoint blockade.
Keywords: Checkpoint blockade; Neoantigens; Oncogene; Predictive biomarkers; T cells.
Conflict of interest statement
Ethics approval and consent to participate
The patients described in this study provided written informed consent as approved by the IRB of Johns Hopkins.
Consent for publication
Not applicable.
Competing interests
K.N.S., F.H., D.M.P, V.A., B.V., K.W.K., N.P., L.A.D, and V.E.V. have filed for patent protection on a subset of the technologies described herein (US provisional application no. 62/407,820). D.M.P. has ownership interest (including patents) in BMS, MedImmune/AstraZeneca, and Potenza, and is a consultant/advisory board member for BMS and MedImmune/AstraZeneca. V.E.V. has ownership interest (including patents) in Personal Genome Diagnostics and is a consultant/advisory board member for the same.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Llosa NJ, Cruise M, Tam A, Wicks EC, Hechenbleikner EM, Taube JM, et al. The vigorous immune microenvironment of microsatellite instable colon cancer is balanced by multiple counter-inhibitory checkpoints. Cancer Discov. 2015;5:43–51. doi: 10.1158/2159-8290.CD-14-0863. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous