

Interatrial block in prediction of all-cause mortality after first-ever ischemic stroke
- PMID: 30744701
- PMCID: PMC6371419
- DOI: 10.1186/s12872-019-1015-5
Interatrial block in prediction of all-cause mortality after first-ever ischemic stroke
Abstract
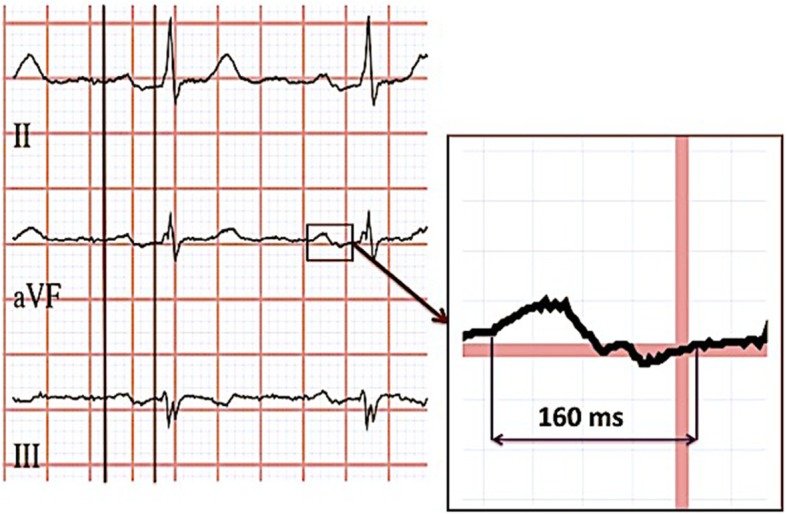
Background: Interatrial block (IAB) is an ECG indicator of atrial fibrosis related to atrial remodeling and thrombus formation thus leading to embolic stroke and increasing mortality. We aimed to assess weather IAB predicted all-cause mortality during 10 years after ischemic stroke.
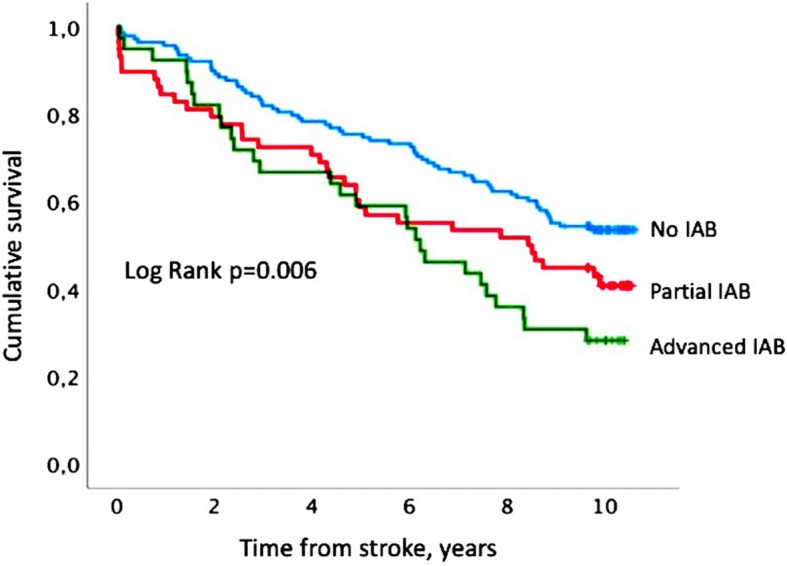
Methods: The study sample comprised 235 patients (median age 74 (interquartile range 25-75% 65-81) years, 95 female) included in the Lund Stroke Register in 2001-2002, who had sinus rhythm ECGs at stroke admission. IAB was defined as a P-wave duration ≥120 ms without = partial IAB (n = 56) or with = advanced IAB (n = 41) biphasic morphology (±) in the inferior ECG leads. All-cause mortality was assessed via linkage with the Swedish Causes of Death Register.
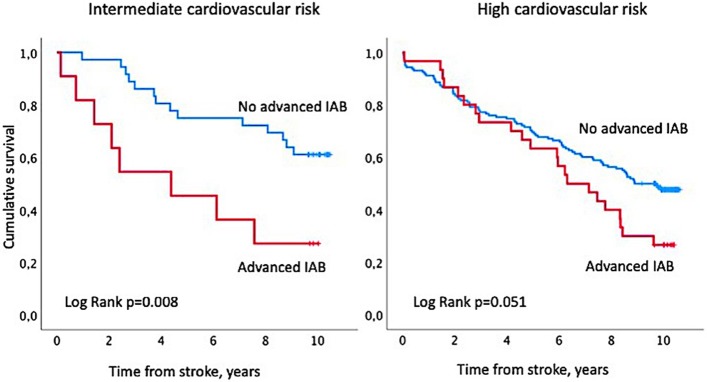
Results: During follow-up 126 patients died (54%). Advanced IAB, but not partial, was associated with all-cause mortality in univariate Cox regression analysis (hazard ratio (HR) 1.98, 95% CI 1.27-3.09, p = 0.003). After adjustment for age, gender, severity of stroke measured by NIHSS scale and smoking status in patients without additional comorbidities advanced IAB independently predicted all-cause mortality (HR 7.89, 95% CI 2.01-30.98, p = 0.003), while in patients with comorbidities it did not (HR 1.01 95% CI 0.59-1.72, p = 0.966).
Conclusion: Advanced IAB predicted all-cause mortality after ischemic stroke, but mostly in patients without additional cardiovascular comorbidities.
Keywords: All-cause mortality; Atrial fibrosis; ECG; Interatrial block; Ischemic stroke.
Conflict of interest statement
Ethics approval and consent to participate
This is a retrospective register-based study based on the data from LSR. Written informed consent was obtained from all participants included in the LSR. The Lund University Ethics Committee approved the study.
Consent for publication
Not applicable as the manuscript does not contain data from any individual person.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bayes de Luna A, Cladellas M, Oter R, Torner P, Guindo J, Marti V, Rivera I, Iturralde P. Interatrial conduction block and retrograde activation of the left atrium and paroxysmal supraventricular tachyarrhythmia. Eur Heart J. 1988;9(10):1112–1118. doi: 10.1093/oxfordjournals.eurheartj.a062407. - DOI - PubMed
-
- Bayes de Luna A, Platonov P, Cosio FG, Cygankiewicz I, Pastore C, Baranowski R, Bayes-Genis A, Guindo J, Vinolas X, Garcia-Niebla J, et al. Interatrial blocks. A separate entity from left atrial enlargement: a consensus report. J Electrocardiol. 2012;45(5):445–451. doi: 10.1016/j.jelectrocard.2012.06.029. - DOI - PubMed
-
- Bernal E, Bayes-Genis A, Ariza-Sole A, Formiga F, Vidan MT, Escobar-Robledo LA, Aboal J, Alcoberro L, Guerrero C, Ariza-Segovia I, et al. Interatrial block, frailty and prognosis in elderly patients with myocardial infarction. J Electrocardiol. 2018;51(1):1–7. doi: 10.1016/j.jelectrocard.2017.08.026. - DOI - PubMed
-
- Magnani JW, Gorodeski EZ, Johnson VM, Sullivan LM, Hamburg NM, Benjamin EJ, Ellinor PT. P wave duration is associated with cardiovascular and all-cause mortality outcomes: the National Health and nutrition examination survey. Heart Rhythm. 2011;8(1):93–100. doi: 10.1016/j.hrthm.2010.09.020. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
