

Drug sensitivity testing on patient-derived sarcoma cells predicts patient response to treatment and identifies c-Sarc inhibitors as active drugs for translocation sarcomas
- PMID: 30745580
- PMCID: PMC6462037
- DOI: 10.1038/s41416-018-0359-4
Drug sensitivity testing on patient-derived sarcoma cells predicts patient response to treatment and identifies c-Sarc inhibitors as active drugs for translocation sarcomas
Abstract
Background: Heterogeneity and low incidence comprise the biggest challenge in sarcoma diagnosis and treatment. Chemotherapy, although efficient for some sarcoma subtypes, generally results in poor clinical responses and is mostly recommended for advanced disease. Specific genomic aberrations have been identified in some sarcoma subtypes but few of them can be targeted with approved drugs.
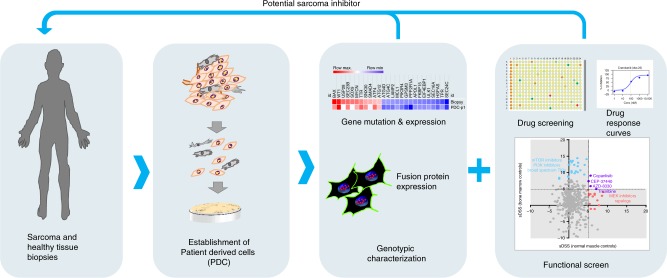
Methods: We cultured and characterised patient-derived sarcoma cells and evaluated their sensitivity to 525 anti-cancer agents including both approved and non-approved drugs. In total, 14 sarcomas and 5 healthy mesenchymal primary cell cultures were studied. The sarcoma biopsies and derived cells were characterised by gene panel sequencing, cancer driver gene expression and by detecting specific fusion oncoproteins in situ in sarcomas with translocations.
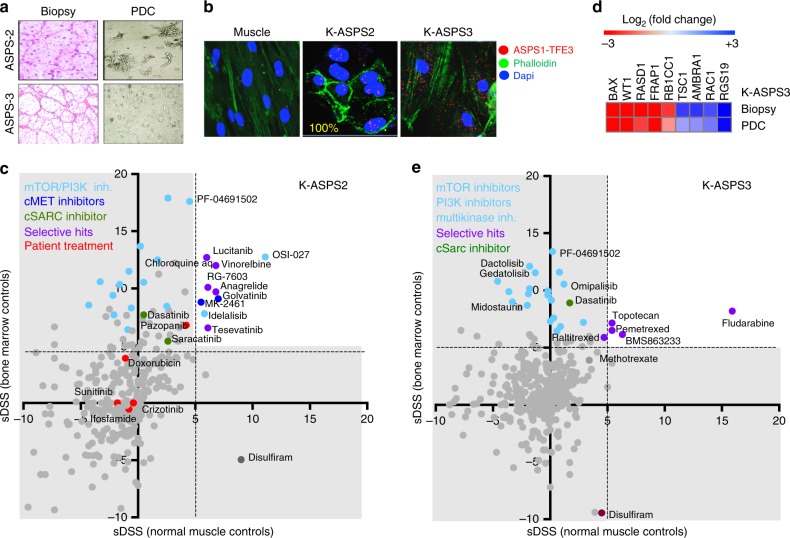
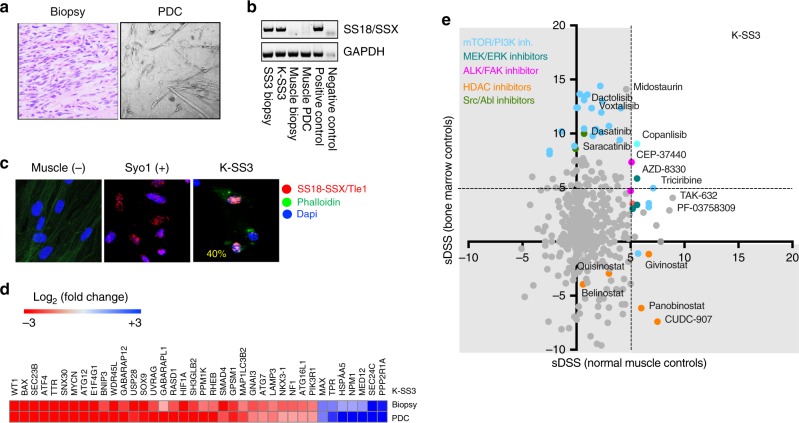
Results: Soft tissue sarcoma cultures were established from patient biopsies with a success rate of 58%. The genomic profile and drug sensitivity testing on these samples helped to identify targeted inhibitors active on sarcomas. The cSrc inhibitor Dasatinib was identified as an active drug in sarcomas carrying chromosomal translocations. The drug sensitivity of the patient sarcoma cells ex vivo correlated with the response to the former treatment of the patient.
Conclusions: Our results show that patient-derived sarcoma cells cultured in vitro are relevant and practical models for genotypic and phenotypic screens aiming to identify efficient drugs to treat sarcoma patients with poor treatment options.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Fletcher, C. D. M., Bridge, J. A., Hogendoorn, P. & Mertens, F. WHO Classification of Tumours of Soft Tissue and Bone 4th edn (IARC Press, Lyon, 2013).
-
- Le Cesne A, et al. Randomized phase III study comparing conventional-dose doxorubicin plus ifosfamide versus high-dose doxorubicin plus ifosfamide plus recombinant human granulocyte-macrophage colony-stimulating factor in advanced soft tissue sarcomas: a trial of the European Organization for Research and Treatment of Cancer/Soft Tissue and Bone Sarcoma Group. J. Clin. Oncol. 2000;18:2676–2684. doi: 10.1200/JCO.2000.18.14.2676. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
