

Difficult Vascular Access Anatomy Associated with Decreased Success of Revascularization in Emergent Thrombectomy
- PMID: 30746003
- PMCID: PMC6350866
Difficult Vascular Access Anatomy Associated with Decreased Success of Revascularization in Emergent Thrombectomy
Abstract
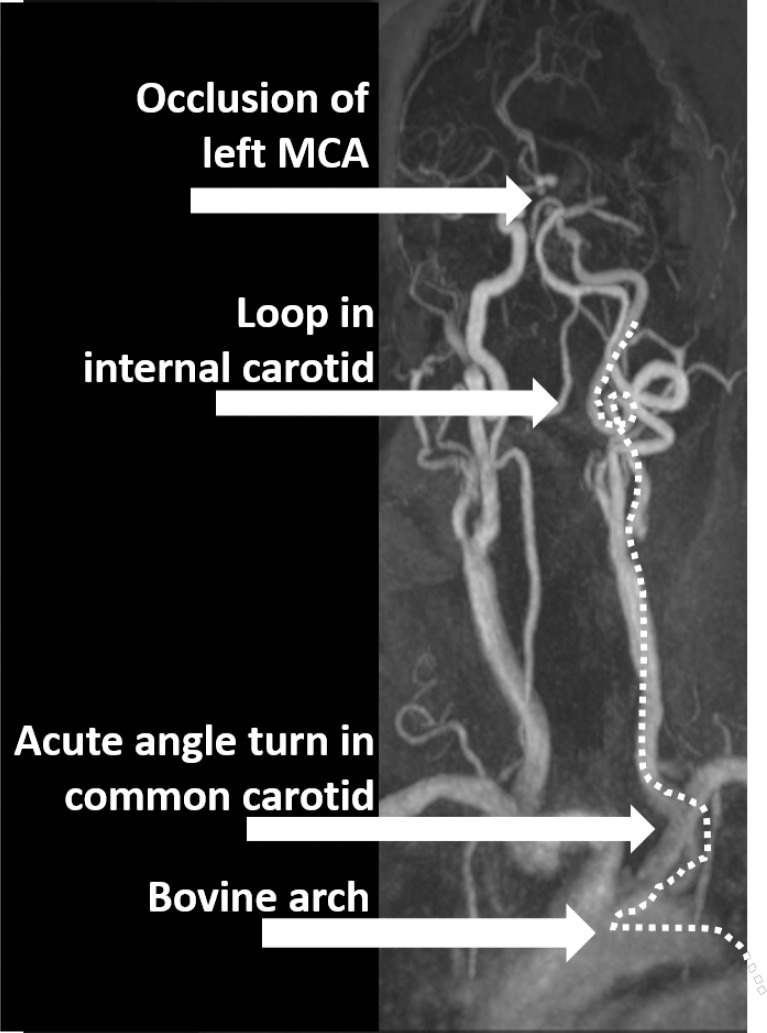
Background: Thrombectomy has become established as a successful treatment strategy for ischemic stroke, and consequently, more patients are undergoing this procedure. Due to comorbid conditions, chronic disease states, and advanced age, many patients have anatomy which complicates revascularization, specifically difficult aortic arch anatomy, or tortuous common and internal artery anatomy, or both.
Methods: In the present study, these unfavorable anatomic parameters were analyzed for 53 patients undergoing acute thrombectomy for ischemic stroke. Statistical analysis was performed and the outcome TICI scores were compared. 26 of the patients analyzed had features of difficult femoral access.
Results: Difficult arch anatomy was associated with unsuccessful revascularization (p = 0.03, Fisher's exact) with only 53% of patients with this feature having favorable TICI scores. Difficult common carotid access was also associated with unsuccessful revascularization (p = 0.004, Fisher's exact) with 38% success. There was a trend toward significance for unsuccessful revascularization for difficult internal carotid artery access (p = 0.06, Fisher's exact).
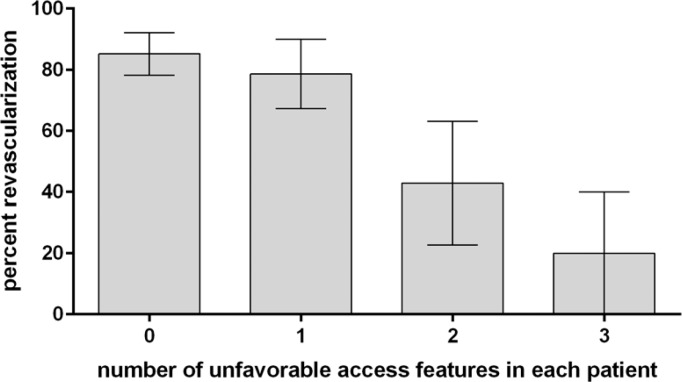
Conclusion: Any combination of the aforementioned anatomic parameters was associated with the decreased success of treatment which was an independent predictor in multivariate analysis (p = 0.009). As difficult access anatomy is commonly encountered in patients undergoing emergent thrombectomy, it is important for the treating physician to be prepared and to adapt access strategies to increase the likelihood of successful revascularization.
Keywords: Thrombectomy; difficult access; ischemic stroke; revascularization.
Figures

References
-
- Dumont TM, et al. Understanding risk factors for perioperative ischemic events with carotid stenting: is patient age over 80 years or is unfavorable arch anatomy to blame? J Neurointerv Surg. 2014;6(3):219–224. - PubMed
-
- Fanous AA, et al. High-risk factors in symptomatic patients undergoing carotid artery stenting with distal protection: Buffalo Risk Assessment Scale (BRASS) Neurosurgery. 2015;77(4):531–542. ; discussion 542–533. - PubMed
-
- Higashida RT, et al. Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke. 2003;34(8):e109–e137. - PubMed
-
- Treurniet KM, et al. Clot burden score on baseline computerized tomographic angiography and intra-arterial treatment effect in acute ischemic stroke. Stroke. 2016;47(12):2972–2978. - PubMed
-
- Puetz V, et al. Intracranial thrombus extent predicts clinical outcome, final infarct size and hemorrhagic transformation in ischemic stroke: the clot burden score. Int J Stroke. 2008;3(4):230–236. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials