

Preoperative 3-dimensional computed tomography lung simulation before video-assisted thoracoscopic anatomic segmentectomy for ground glass opacity in lung
- PMID: 30746205
- PMCID: PMC6344718
- DOI: 10.21037/jtd.2018.10.126
Preoperative 3-dimensional computed tomography lung simulation before video-assisted thoracoscopic anatomic segmentectomy for ground glass opacity in lung
Abstract
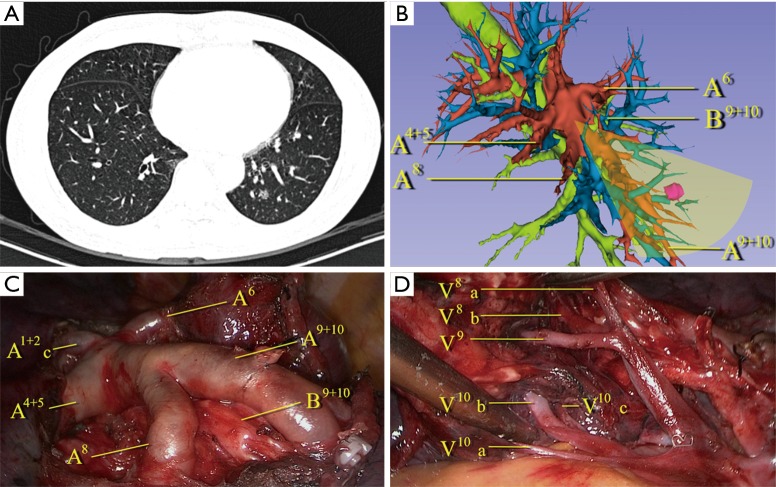
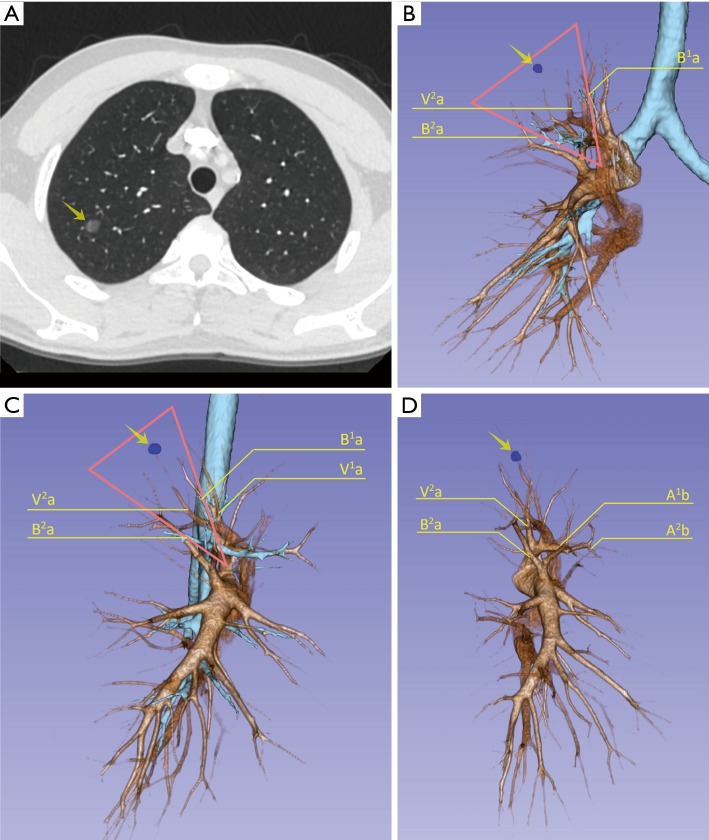
Background: Three-dimensional (3D) simulation of pulmonary vessels and the space between the lesion and adjacent tissues may improve the safety and accuracy of video-assisted thoracoscopic surgery (VATS) for lung. The aim of this study was to evaluate the effect of 3D simulation on the outcome of VATS segmentectomy for ground glass opacity (GGO) in lung.
Methods: We retrospectively analyzed 68 cases of small (≤2 cm) GGO, which were diagnosed as cT1aN0M0 lung cancer, from May 1, 2016 to February 28, 2017 in our institute. All the patients underwent VATS segmentectomy. The patients were divided into "3D" group, 3D preoperative reconstruction simulation in 36 patients and "non-3D" group, 32 patients with only computed tomography (CT). Operation plans were firstly made by CT in all patients, then by 3D simulation only in 3D group. The clinical outcomes, including operation time, blood loss, resection margin distance, length of postoperative stay and postoperative complications were compared between the two groups.
Results: There were 21 male and 47 female analyzed, aging from 34 to 72 years (median 57). In 3D group, pathological result showed 8 cases of adenocarcinoma, 23 cases of microinvasive adenocarcinoma (MIA), 5 cases of adenocarcinoma in situ (AIS). In non-3D group, 18 cases of MIA, 9 cases of adenocarcinoma and 5 cases of AIS were diagnosed pathologically. The blood loss, postoperative hospital stay and the incidence of the postoperative complications were similar in both of the groups. There was no 30-day postoperative mortality in either group. The median operation time for the 3D group (111 minute) was shorter than non-3D group (139 minute) (P=0.03). Seven cases (19%) in 3D group changed the original operation plan according to the simulation result with the consideration of adequate resection margin distance. All cases in 3D group had adequate resection margin distance. Four cases (13%) in non-3D group got inadequate resection margin distance, and more lung tissues than the original plan were then resected in these patients (P=0.04).
Conclusions: 3D preoperative simulation may be more precise in operation plan than CT scan and can significantly shorten the operation time in VATS segmentectomy for GGO in lung.
Keywords: Video-assisted thoracoscopic surgery (VATS); lung cancer; segmentectomy; three-dimensional simulation (3D simulation).
Conflict of interest statement
Conflicts of Interest: This study was presented at the 31st EACTS Annual Meeting, 7-11 October 2017, in Vienna, Austria.
Figures
References
LinkOut - more resources
Full Text Sources
Medical