

Mobile Digital Education for Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration
- PMID: 30747711
- PMCID: PMC6390189
- DOI: 10.2196/12937
Mobile Digital Education for Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration
Abstract
Background: There is a pressing need to implement efficient and cost-effective training to address the worldwide shortage of health professionals. Mobile digital education (mLearning) has been mooted as a potential solution to increase the delivery of health professions education as it offers the opportunity for wide access at low cost and flexibility with the portability of mobile devices. To better inform policy making, we need to determine the effectiveness of mLearning.
Objective: The primary objective of this review was to evaluate the effectiveness of mLearning interventions for delivering health professions education in terms of learners' knowledge, skills, attitudes, and satisfaction.
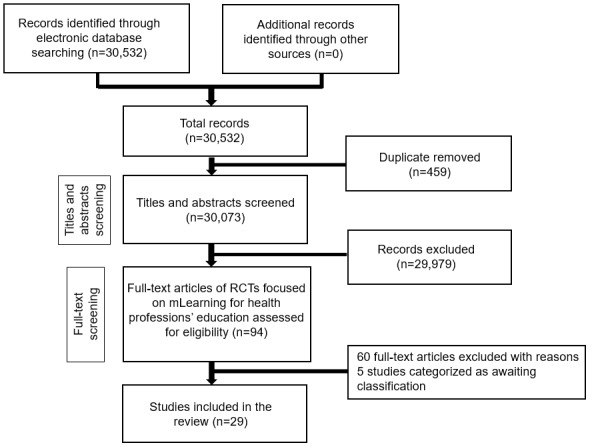
Methods: We performed a systematic review of the effectiveness of mLearning in health professions education using standard Cochrane methodology. We searched 7 major bibliographic databases from January 1990 to August 2017 and included randomized controlled trials (RCTs) or cluster RCTs.
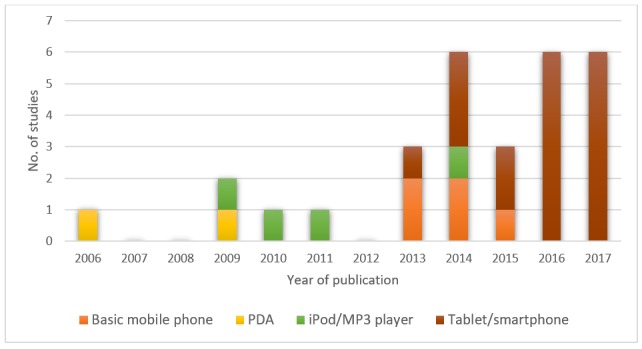
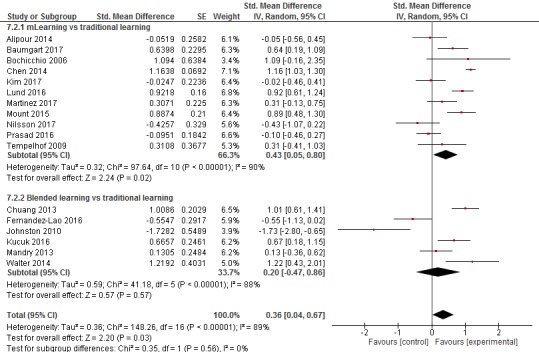
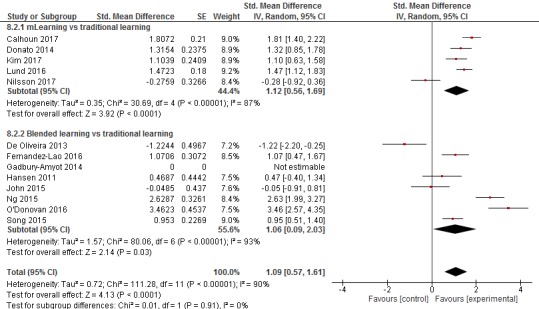
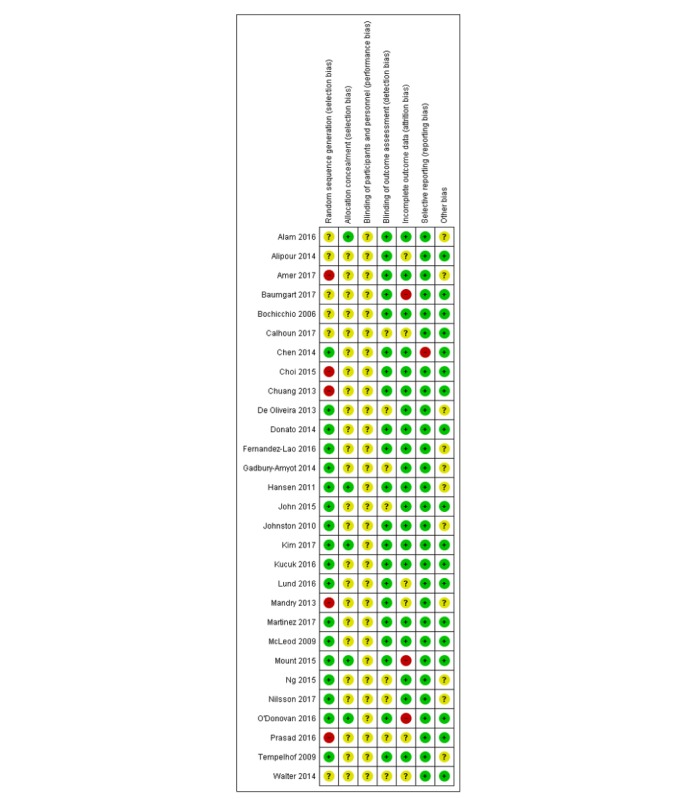
Results: A total of 29 studies, including 3175 learners, met the inclusion criteria. A total of 25 studies were RCTs and 4 were cluster RCTs. Interventions comprised tablet or smartphone apps, personal digital assistants, basic mobile phones, iPods, and Moving Picture Experts Group-1 audio layer 3 player devices to deliver learning content. A total of 20 studies assessed knowledge (n=2469) and compared mLearning or blended learning to traditional learning or another form of digital education. The pooled estimate of studies favored mLearning over traditional learning for knowledge (standardized mean difference [SMD]=0.43, 95% CI 0.05-0.80, N=11 studies, low-quality evidence). There was no difference between blended learning and traditional learning for knowledge (SMD=0.20, 95% CI -0.47 to 0.86, N=6 studies, low-quality evidence). A total of 14 studies assessed skills (n=1097) and compared mLearning or blended learning to traditional learning or another form of digital education. The pooled estimate of studies favored mLearning (SMD=1.12, 95% CI 0.56-1.69, N=5 studies, moderate quality evidence) and blended learning (SMD=1.06, 95% CI 0.09-2.03, N=7 studies, low-quality evidence) over traditional learning for skills. A total of 5 and 4 studies assessed attitudes (n=440) and satisfaction (n=327), respectively, with inconclusive findings reported for each outcome. The risk of bias was judged as high in 16 studies.
Conclusions: The evidence base suggests that mLearning is as effective as traditional learning or possibly more so. Although acknowledging the heterogeneity among the studies, this synthesis provides encouraging early evidence to strengthen efforts aimed at expanding health professions education using mobile devices in order to help tackle the global shortage of health professionals.
Keywords: digital education; health workforce; mLearning; meta-analysis; systematic review.
©Gerard Dunleavy, Charoula Konstantia Nikolaou, Sokratis Nifakos, Rifat Atun, Gloria Chun Yi Law, Lorainne Tudor Car. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 12.02.2019.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Horton R, Araujo ES, Bhorat H, Bruysten S, Jacinto CG, McPake B, Reddy KS, Reinikka R, Schmidt JO, Song L, Tangcharoensathien V, Trent-Adams S, Weakliam D, Yamin AE. World Health Organization. 2016. Mar 2, [2018-10-01]. Final report of the expert group to the High-Level Commission on Health Employment and Economic Growth https://www.who.int/hrh/com-heeg/reports/report-expert-group/en/
-
- World Health Organization. 2014. [2017-12-11]. Health Workforce 2030: A global strategy on human resources for health http://www.who.int/workforcealliance/knowledge/resources/strategy_brochu... .
-
- Nair M, Webster P. Health professionals' migration in emerging market economies: patterns, causes and possible solutions. J Public Health (Oxf) 2013 Mar;35(1):157–63. doi: 10.1093/pubmed/fds087. https://academic.oup.com/jpubhealth/article/35/1/157/1592927 - DOI - PubMed
-
- Chen LC. Striking the right balance: health workforce retention in remote and rural areas. Bull World Health Organ. 2010 May;88(5):323. doi: 10.2471/BLT.10.078477. https://www.who.int/bulletin/volumes/88/5/10-078477.pdf - DOI - PMC - PubMed
-
- Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T, Fineberg H, Garcia P, Ke Y, Kelley P, Kistnasamy B, Meleis A, Naylor D, Pablos-Mendez A, Reddy S, Scrimshaw S, Sepulveda J, Serwadda D, Zurayk H. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The Lancet. 2010 Dec 4;376(9756):1923–58. doi: 10.1016/S0140-6736(10)61854-5. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
