

Use of Aspergillus fumigatus real-time PCR in bronchoalveolar lavage samples (BAL) for diagnosis of invasive aspergillosis, including azole-resistant cases, in high risk haematology patients: the need for a combined use with galactomannan
- PMID: 30753590
- PMCID: PMC7107636
- DOI: 10.1093/mmy/myz002
Use of Aspergillus fumigatus real-time PCR in bronchoalveolar lavage samples (BAL) for diagnosis of invasive aspergillosis, including azole-resistant cases, in high risk haematology patients: the need for a combined use with galactomannan
Abstract
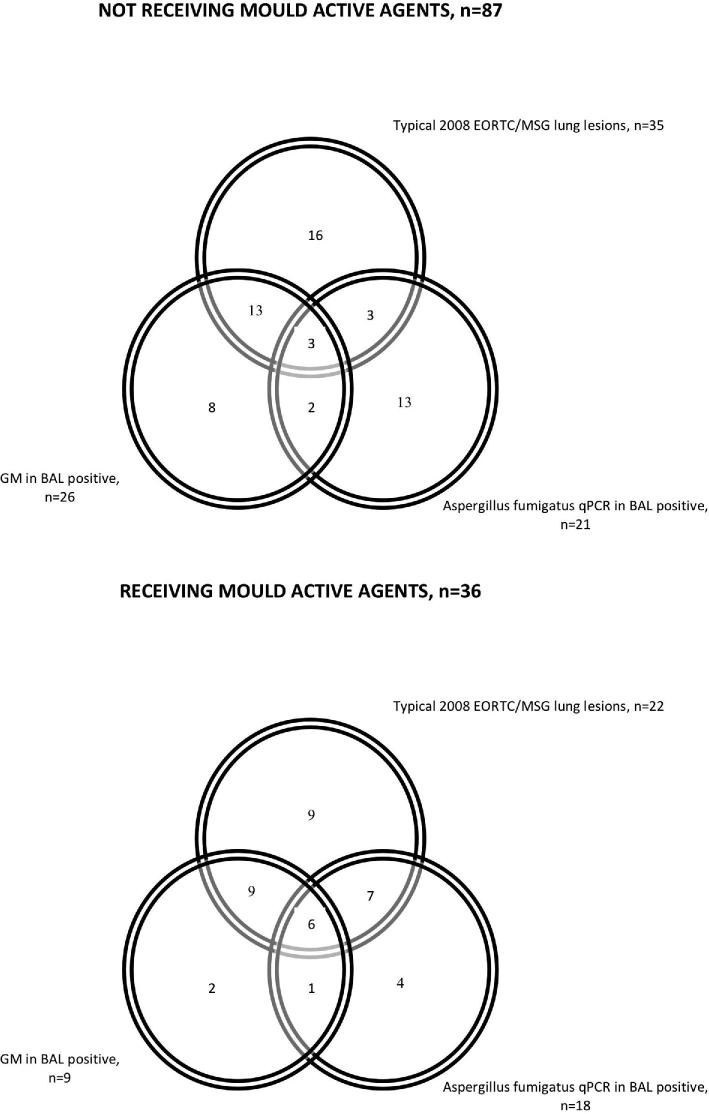
Diagnosis of invasive aspergillosis (IA) is challenging, particularly in high-risk patients with lung lesions other than typical according to 2008-EORTC/MSG criteria. Even if microbiology is positive, they still remain unclassified according to 2008-EORTC/MSG. Quantitative polymerase chain reaction (qPCR) provides new mycological documentation of IA. This retrospective study assessed Aspergillus fumigatus real time qPCR (MycoGENIE®) in BAL to diagnose IA and identify azole-resistant strains. Clinical, radiological, and microbiological data from 114 hematology patients (69% HSCT recipients; 29% on mould active agents) from years 2012-2017 were collected; and 123 BAL samples were tested with qPCR (cutoff: Ct < 40) and galactomannan (GM, Platelia®, cutoff: 0.5 ODI). Patients were classified as proven/probable, possible, and no-IA. "Atypical-IA" referred to patients with lesions other than typical according to 2008-EORTC/MSG and positive mycology. Proven IA was diagnosed in two cases (1.6%), probable in 28 (22.8%), possible in 27 (22%), atypical in 14 (11.4%). qPCR was positive in 39 samples (31.7%). Sensitivity and specificity of qPCR for proven/probable IA (vs no-IA; atypical-IA excluded) were 40% (95% confidence interval [CI]: 23-59) and 69% (95%CI: 55-81), respectively. Sensitivity of qPCR was higher when combined with GM (83%, 95%CI: 65-94) and in those receiving mould-active agents at BAL (61%, 95%CI: 32-86). One sample had TR34/L98H mutation. In conclusion, in high-risk hematology patients with various lung lesions, A. fumigatus qPCR in BAL contributes to diagnosing IA, particularly if combined with GM and in patients receiving mould-active agents might allow detecting azole-resistant mutations in culture negative samples.
Keywords: Aspergillus fumigatus PCR; BAL; HSCT; galactomannan; invasive aspergillosis.
© The Author(s) 2019. Published by Oxford University Press on behalf of The International Society for Human and Animal Mycology.
Figures
References
-
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015; 70: 270–277. - PubMed
-
- Ullmann AJ, Aguado JM, Arikan-Akdagli S et al.. Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin Microbiol Infect. 2018; 24: e1–e38. - PubMed
