

Increased risk of pseudoprogression among pediatric low-grade glioma patients treated with proton versus photon radiotherapy
- PMID: 30753704
- PMCID: PMC6502497
- DOI: 10.1093/neuonc/noz042
Increased risk of pseudoprogression among pediatric low-grade glioma patients treated with proton versus photon radiotherapy
Abstract
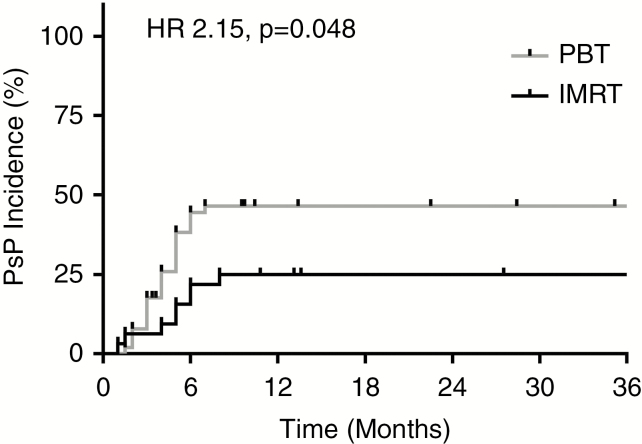
Background: Pseudoprogression (PsP) is a recognized phenomenon after radiotherapy (RT) for high-grade glioma but is poorly characterized for low-grade glioma (LGG). We sought to characterize PsP for pediatric LGG patients treated with RT, with particular focus on the role of RT modality using photon-based intensity-modulated RT (IMRT) or proton beam therapy (PBT).
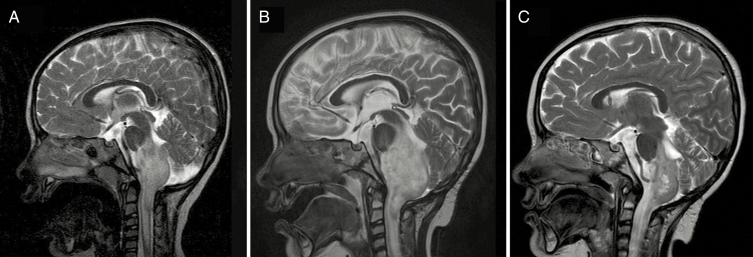
Methods: Serial MRI scans from 83 pediatric LGG patients managed at 2 institutions between 1998 and 2017 were evaluated. PsP was scored when a progressive lesion subsequently decreased or stabilized for at least a year without therapy.
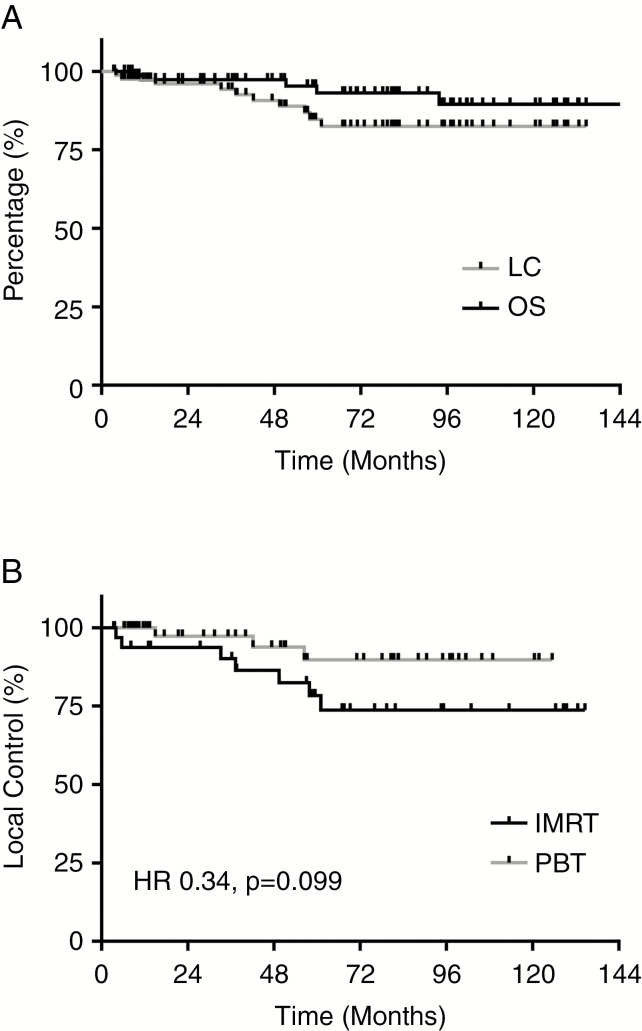
Results: Thirty-two patients (39%) were treated with IMRT, and 51 (61%) were treated with PBT. Median RT dose for the cohort was 50.4 Gy(RBE) (range, 45-59.4 Gy[RBE]). PsP was identified in 31 patients (37%), including 8/32 IMRT patients (25%) and 23/51 PBT patients (45%). PBT patients were significantly more likely to have post-RT enlargement (hazard ratio [HR] 2.15, 95% CI: 1.06-4.38, P = 0.048). RT dose >50.4 Gy(RBE) similarly predicted higher rates of PsP (HR 2.61, 95% CI: 1.20-5.68, P = 0.016). Multivariable analysis confirmed the independent effects of RT modality (P = 0.03) and RT dose (P = 0.01) on PsP incidence. Local progression occurred in 10 patients: 7 IMRT patients (22%) and 3 PBT patients (6%), with a trend toward improved local control for PBT patients (HR 0.34, 95% CI: 0.10-1.18, P = 0.099).
Conclusions: These data highlight substantial rates of PsP among pediatric LGG patients, particularly those treated with PBT. PsP should be considered when assessing response to RT in LGG patients within the first year after RT.
Keywords: low-grade glioma; pediatric malignancy; proton beam therapy; pseudoprogression; radiotherapy.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Pseudoprogression in low-grade glioma.Transl Cancer Res. 2019 Dec;8(Suppl 6):S580-S584. doi: 10.21037/tcr.2019.11.16. Transl Cancer Res. 2019. PMID: 35117135 Free PMC article. No abstract available.
References
-
- Packer RJ, Ater J, Allen J, et al. Carboplatin and vincristine chemotherapy for children with newly diagnosed progressive low-grade gliomas. J Neurosurg. 1997;86(5):747–754. - PubMed
-
- Gnekow AK, Falkenstein F, von Hornstein S, et al. Long-term follow-up of the multicenter, multidisciplinary treatment study HIT-LGG-1996 for low-grade glioma in children and adolescents of the German Speaking Society of Pediatric Oncology and Hematology. Neuro Oncol. 2012;14(10):1265–1284. - PMC - PubMed
-
- Paulino AC, Mazloom A, Terashima K, et al. Intensity-modulated radiotherapy (IMRT) in pediatric low-grade glioma. Cancer. 2013;119(14): 2654–2659. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
