

Intraductal tubular papillary neoplasm (ITPN), a novel entity of pancreatic epithelial neoplasms and precursor of cancer: A case report and review of the literature
- PMID: 30753991
- PMCID: PMC6370588
- DOI: 10.1016/j.ijscr.2019.01.036
Intraductal tubular papillary neoplasm (ITPN), a novel entity of pancreatic epithelial neoplasms and precursor of cancer: A case report and review of the literature
Abstract
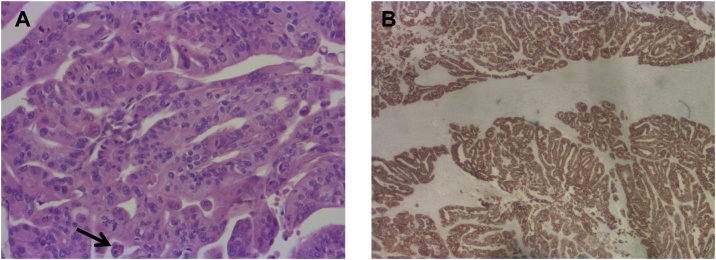
Background: Intraductal tubular papillary neoplasm (ITPN) displays a very rare subtype of epithelial neoplasms of the pancreas. ITPN is characterized by intraductal tubulopapillary growth and cellular dysplasia. In contrast to intraductal papillary neoplasm (IPMN) no overt epithelial mucin production is observed. To date, little is known about ITPN and particularly about pancreatic cancer arising in this tumor entity.
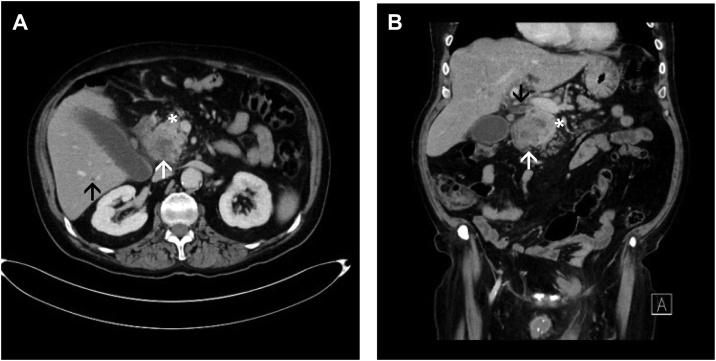
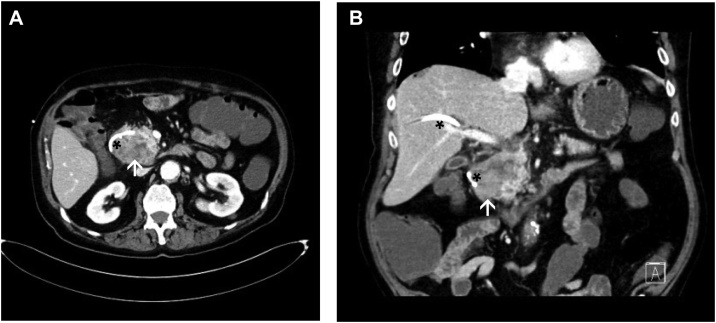
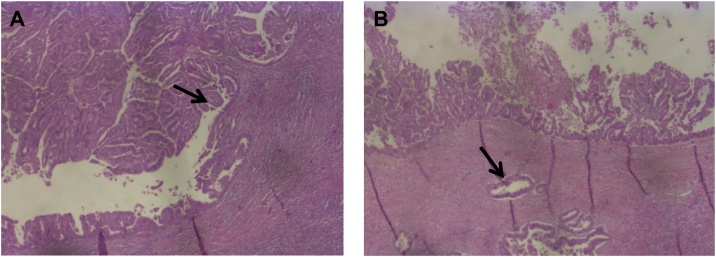
Case presentation: A 68-year-old male presented at our hospital with a distal bile duct occlusion suspicious for adenocarcinoma of the pancreatic head. Preoperative staging revealed no signs of distant metastasis. The patient was surgically explored and pylorus preserving duodenopancreatectomy was performed for a solid pancreatic head tumor. Final histopathology surprisingly revealed an ITPN with an associated invasive carcinoma pT3, pN0 (0/12), R0, G2.
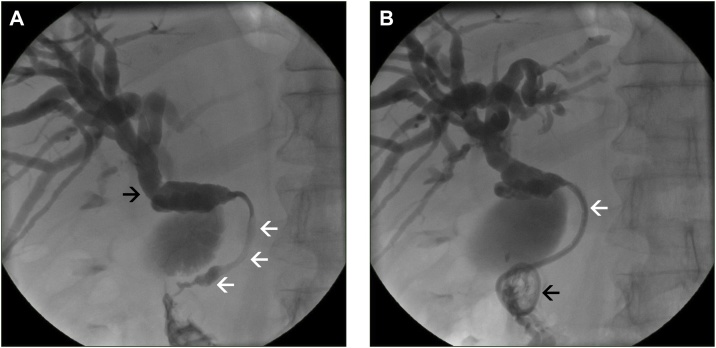
Discussion: Patients with ITPN frequently present with jaundice suspicious for a bile duct stenosis or a malignant tumor of the pancreatic head. Although, it is possible to diagnose ITPN by endoscopic retrograde cholangiopancreaticography, many tumors are found not before histopathological examination. Differential diagnosis includes ductal adenocarcinoma of the pancreas, neuroendocrine tumors, IPMN, distal bile duct tumors, and solid pseudopapillary neoplasms. Using immunohistochemistry, other entities of pancreatic tumors can be ruled out. In case of R0 resection oncological prognosis is described to be more favorable when compared to regular ductal adenocarcinoma.
Conclusion: ITPN displays a rare entity of pancreatic neoplasms. As shown in the present case report, there is a relevant potential of malignant transformation and therefore radical surgical resection and oncologic follow-up is warranted.
Keywords: Cancer risk; Cystic tumors of the pancreas; ITPN; Intraductal tubular papillary neoplasm; Pancreas.
Copyright © 2019 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures
Similar articles
-
Intraductal tubulopapillary neoplasm (ITPN) of the pancreas associated with an invasive component: a case report with review of the literature.World J Surg Oncol. 2017 Nov 16;15(1):203. doi: 10.1186/s12957-017-1267-4. World J Surg Oncol. 2017. PMID: 29145864 Free PMC article. Review.
-
[A rare case of intraductal tumor of the pancreas in which an intraductal tubulopapillary neoplasm was mixed with a widely spreading gastric-type intraductal papillary-mucinous neoplasm].Nihon Shokakibyo Gakkai Zasshi. 2024;121(5):415-424. doi: 10.11405/nisshoshi.121.415. Nihon Shokakibyo Gakkai Zasshi. 2024. PMID: 38735750 Japanese.
-
A case of intraductal tubulopapillary neoplasm of the pancreas in a branch duct: a rare case report and literature review.BMC Gastroenterol. 2021 Apr 13;21(1):162. doi: 10.1186/s12876-021-01744-2. BMC Gastroenterol. 2021. PMID: 33849435 Free PMC article. Review.
-
Concurrent presentation of an intraductal tubulopapillary neoplasm and intraductal papillary mucinous neoplasm in the branch duct of the pancreas, with a superior mesenteric artery aneurysm: a case report.World J Surg Oncol. 2018 Apr 24;16(1):83. doi: 10.1186/s12957-018-1391-9. World J Surg Oncol. 2018. PMID: 29690869 Free PMC article.
-
An extremely rare case who underwent total remnant pancreatectomy due to recurrent pancreatic metastasis of intraductal tubulopapillary neoplasm.Clin J Gastroenterol. 2019 Apr;12(2):153-159. doi: 10.1007/s12328-018-0913-x. Epub 2018 Oct 4. Clin J Gastroenterol. 2019. PMID: 30284703
Cited by
-
Imaging features of intraductal tubulopapillary neoplasm of the pancreas and its differentiation from conventional pancreatic ductal adenocarcinoma.Sci Rep. 2022 Sep 16;12(1):15557. doi: 10.1038/s41598-022-19517-6. Sci Rep. 2022. PMID: 36114217 Free PMC article.
-
Intraductal tubulopapillary neoplasm (ITPN) of the pancreas: a distinct entity among pancreatic tumors.Histopathology. 2022 Sep;81(3):297-309. doi: 10.1111/his.14698. Epub 2022 May 27. Histopathology. 2022. PMID: 35583805 Free PMC article.
-
Intraductal Tubulopapillary Neoplasm of the Pancreas Presenting as a Localized Pancreatic Tumor in a 52-Year-Old Woman: Focusing on a Rare Pancreatic Malignancy and Contrasting to Intrapapillary Mucinous Neoplasm.Cureus. 2020 Jun 10;12(6):e8548. doi: 10.7759/cureus.8548. Cureus. 2020. PMID: 32670685 Free PMC article.
-
Rapid transformation of branched pancreatic duct-derived intraductal tubulopapillary neoplasm into an invasive carcinoma: A case report.World J Clin Oncol. 2023 Dec 24;14(12):620-627. doi: 10.5306/wjco.v14.i12.620. World J Clin Oncol. 2023. PMID: 38179403 Free PMC article.
-
Real-Life Management of Pancreatic Cysts: Simplified Review of Current Guidelines.J Clin Med. 2023 Jun 13;12(12):4020. doi: 10.3390/jcm12124020. J Clin Med. 2023. PMID: 37373713 Free PMC article. Review.
References
-
- Yamaguchi H., Shimizu M., Ban S. Intraductal tubulopapillary neoplasms of the pancreas distinct from pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am. J. Surg. Pathol. 2009;33(8):1164–1172. - PubMed
-
- Adsay N.V., Fukushima N., Furukawa T. In: Intraductal Neoplasms of the Pancreas in WHO Classification of Tumor of the Digestive System. Bosman F.T., Carneiro F., Hruban R.H., Theise N.D., editors. IARC; Lyon: 2010. 2010.
-
- Tanaka M., Fernandez-Del Castillo C., Kamisawa T. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017;17(5):738–753. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
