

Full versus half dose of antenatal betamethasone to prevent severe neonatal respiratory distress syndrome associated with preterm birth: study protocol for a randomised, multicenter, double blind, placebo-controlled, non-inferiority trial (BETADOSE)
- PMID: 30755164
- PMCID: PMC6373166
- DOI: 10.1186/s12884-019-2206-x
Full versus half dose of antenatal betamethasone to prevent severe neonatal respiratory distress syndrome associated with preterm birth: study protocol for a randomised, multicenter, double blind, placebo-controlled, non-inferiority trial (BETADOSE)
Abstract
Background: Although antenatal betamethasone is recommended worldwide for women at risk of preterm delivery, concerns persist regarding the long-term effects associated with this treatment. Indeed, adverse events, mainly dose-related, have been reported. The current recommended dose of antenatal betamethasone directly derives from sheep experiments performed in the late 60's and has not been challenged in 45 years. Therefore, randomized trials evaluating novel dose regimens are urgently needed.
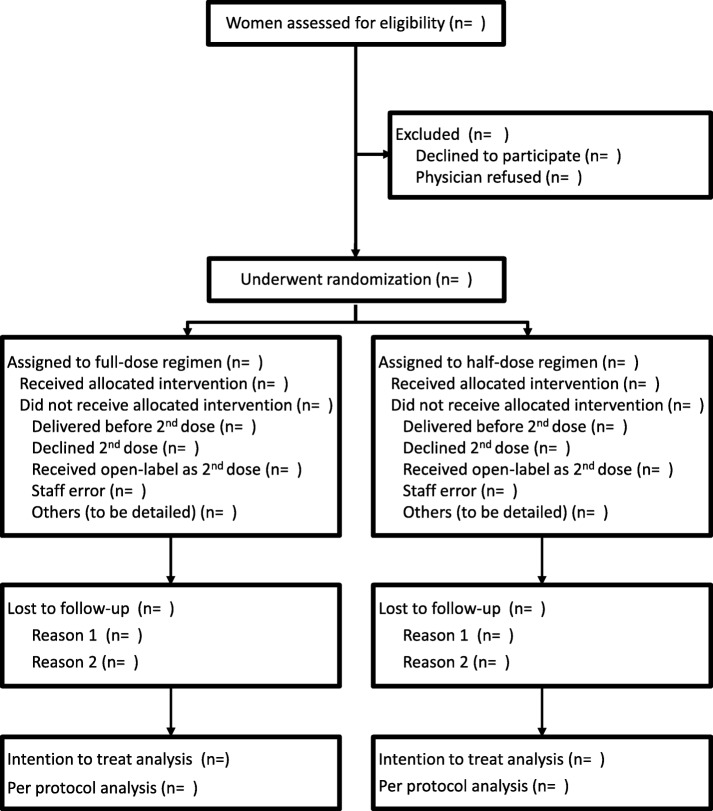
Methods: A randomised, double blind, placebo-controlled, non-inferiority trial will be performed in 37 French level 3 maternity units. Women with a singleton pregnancy at risk of preterm delivery before 32 weeks of gestation having already received a first 11.4 mg injection of betamethasone will be randomised to receive either a second injection of 11.4 mg betamethasone (full dose arm) or placebo (half dose arm) administered intramuscularly 24 h after the first injection. The primary binary outcome will be the occurrence of severe respiratory distress syndrome (RDS), defined as the need for exogenous intra-tracheal surfactant in the first 48 h of life. Considering that 20% of the pregnant women receiving the full dose regimen would have a neonate with severe RDS, 1571 patients in each treatment group are required to show that the half dose regimen is not inferior to the full dose, that is the difference in severe RDS rate do not exceed 4% (corresponding to a Relative Risk of 20%), with a 1-sided 2.5% type-1 error and a 80% power. Interim analyses will be done after every 300 neonates who reach the primary outcome on the basis of intention-to-treat, using a group-sequential non-inferiority design.
Discussion: If the 50% reduced antenatal betamethasone dose is shown to be non-inferior to the full dose to prevent severe RDS associated with preterm birth, then it should be used consistently in women at risk of preterm delivery and would be of great importance to their children.
Trial registration: ClinicalTrials.gov identifier: NCT 02897076 (registration date 09/13/2016).
Trial registration: ClinicalTrials.gov NCT02897076.
Keywords: Antenatal betamethasone; Antenatal corticosteroids; Non-inferiority; Preterm birth; Preterm delivery; Respiratory distress syndrome.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was granted by the Committee for the Protection of People participating to biomedical research Ile-de-France 1 (#14242ND, June, 26th 2016) and the National Agency for Drug Security (#160457A-22, May, 25th 2016). Women were included and randomized in the BETADOSE trial only after written informed consent to participate was obtained.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- Liggins GC, Higgins RN. A controlled trial of antepartum glucocorticoid treatment for prevention of the respiratory distress syndrome in premature infants. Pediatrics. 1972;50:515–525. - PubMed
-
- National Institutes of Health Consensus Development Conference Statement Effect of corticosteroids for fetal maturation on perinatal outcomes. Am J Obstet Gynecol. 1995;173:246–252. doi: 10.1016/0002-9378(95)90208-2. - DOI
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
