

L-shaped corticotomy with bone flap sliding in the management of chronic tibial osteomyelitis: surgical technique and clinical results
- PMID: 30755228
- PMCID: PMC6373117
- DOI: 10.1186/s13018-019-1086-0
L-shaped corticotomy with bone flap sliding in the management of chronic tibial osteomyelitis: surgical technique and clinical results
Abstract
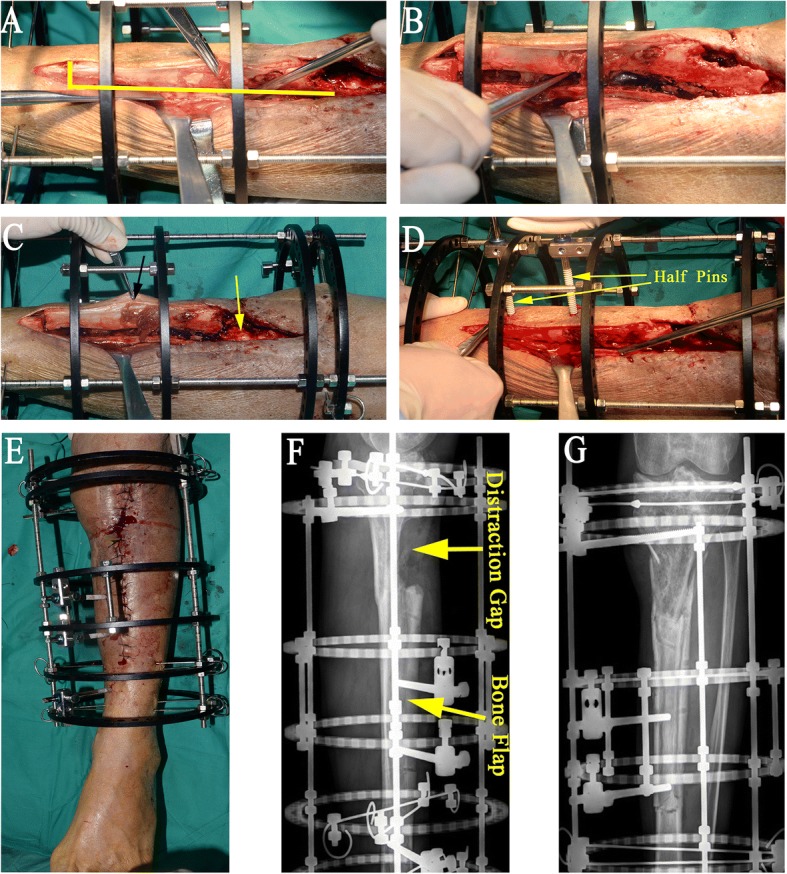
Background: We described the use of the technique of L-shaped corticotomy with bone flap sliding to treat chronic osteomyelitis of the tibia in eight patients and presented the preliminary results.
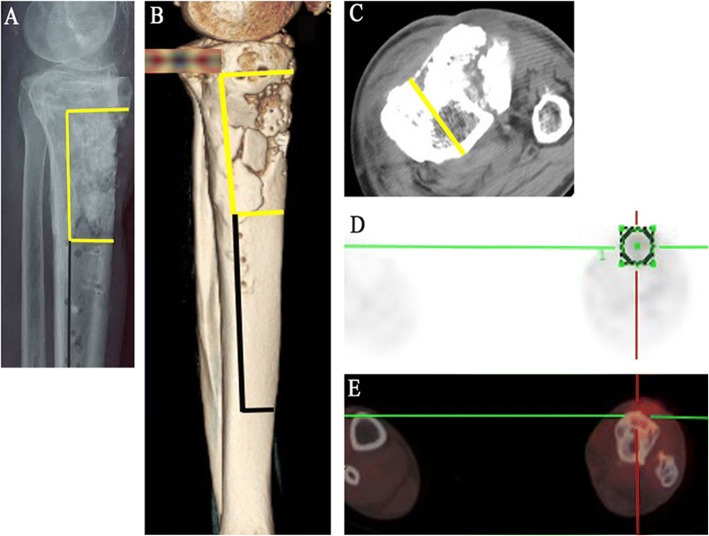
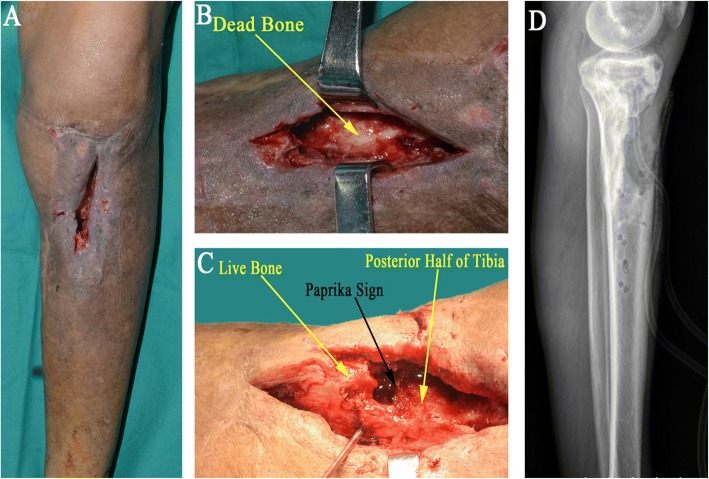
Methods: L-shaped corticotomy with bone flap sliding was performed in eight patients between 2007 and 2014. All patients had chronic tibial osteomyelitis involving the anterior tibial cortex with intact and healthy posterior cortex. The size of bone defects following sequestrectomy and radical debridement was 8.1 cm on average. One patient required a latissimus dorsi flap. The mean follow-up period was 34.1 months. The functional and bone results were evaluated at the time of the latest follow-up.
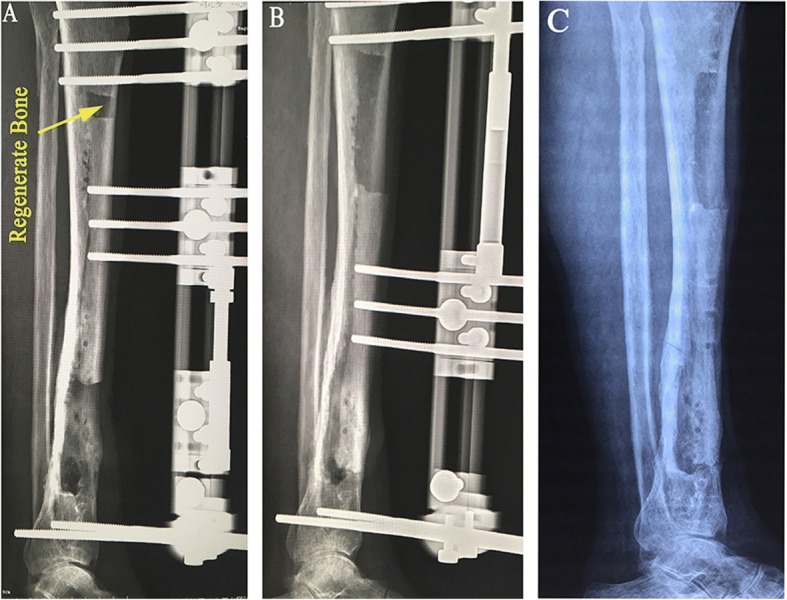
Results: Complete eradication of infection and union of docking sites were achieved in all patients. Functional results were judged excellent in five patients and good in the rest three patients. Bone results were graded as excellent in all cases. The mean external fixation time was 169.9 days and external fixation index was 21.2 days/cm. Pain was the most common complaint that we faced during lengthening. Pin tract infections were observed in four patients, and mild transient stiffness of ankle joint was observed in three patients.
Conclusions: We have found this technique to be safe and effective, significantly diminishing the external fixation index. The earlier removal of the external fixator may result in increased patient comfort, a reduced complication rate, and a rapid and convenient rehabilitation.
Keywords: Bone flap; Bone transport; L-shaped corticotomy; Tibial osteomyelitis.
Conflict of interest statement
Ethics approval and consent to participate
This study are approved by the Ethics Committee of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. Informed consent for participation was obtained from all participants in this study.
Consent for publication
All consents to publish from the patients who took part in this study were obtained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
