

DeepSOFA: A Continuous Acuity Score for Critically Ill Patients using Clinically Interpretable Deep Learning
- PMID: 30755689
- PMCID: PMC6372608
- DOI: 10.1038/s41598-019-38491-0
DeepSOFA: A Continuous Acuity Score for Critically Ill Patients using Clinically Interpretable Deep Learning
Abstract
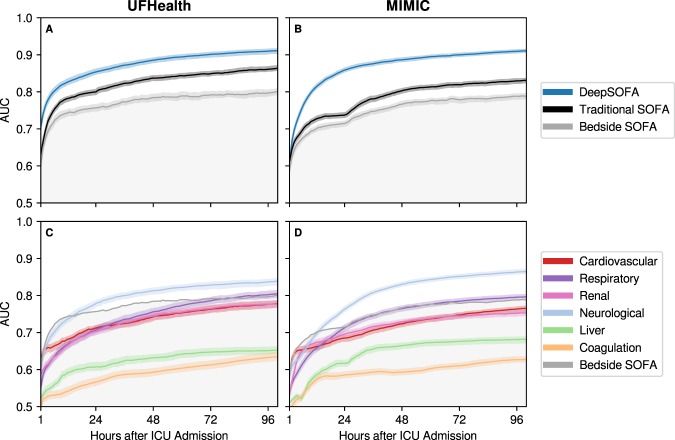
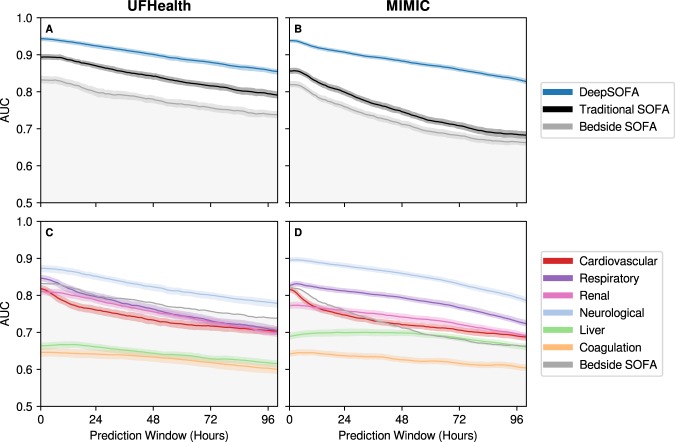
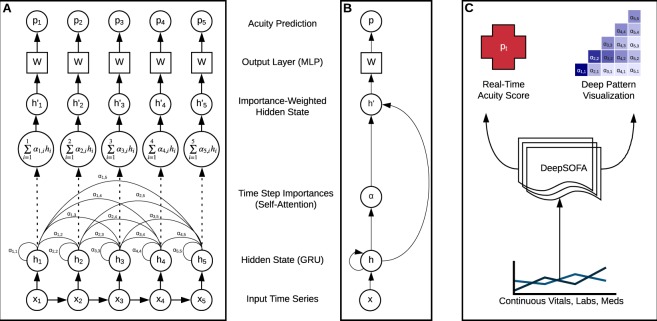
Traditional methods for assessing illness severity and predicting in-hospital mortality among critically ill patients require time-consuming, error-prone calculations using static variable thresholds. These methods do not capitalize on the emerging availability of streaming electronic health record data or capture time-sensitive individual physiological patterns, a critical task in the intensive care unit. We propose a novel acuity score framework (DeepSOFA) that leverages temporal measurements and interpretable deep learning models to assess illness severity at any point during an ICU stay. We compare DeepSOFA with SOFA (Sequential Organ Failure Assessment) baseline models using the same model inputs and find that at any point during an ICU admission, DeepSOFA yields significantly more accurate predictions of in-hospital mortality. A DeepSOFA model developed in a public database and validated in a single institutional cohort had a mean AUC for the entire ICU stay of 0.90 (95% CI 0.90-0.91) compared with baseline SOFA models with mean AUC 0.79 (95% CI 0.79-0.80) and 0.85 (95% CI 0.85-0.86). Deep models are well-suited to identify ICU patients in need of life-saving interventions prior to the occurrence of an unexpected adverse event and inform shared decision-making processes among patients, providers, and families regarding goals of care and optimal resource utilization.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Vincent JL, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–710. - PubMed
-
- Ferreira F, Bota D, Bross A, Mélot C, Vincent J. Serial evaluation of the sofa score to predict outcome in critically ill patients. J. Am. Med. Assoc. 2001;286:1754–1758. - PubMed
-
- Vincent J-L, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units. Crit. Care Med. 1998;26:1793–1800. - PubMed
-
- Badawi O, Liu X, Hassan E, Amelung PJ, Swami S. Evaluation of ICU Risk Models Adapted for Use as Continuous Markers of Severity of Illness Throughout the ICU Stay. Crit. Care Med. 2018;46:361–367. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
