

Brodie's Abscess: A Systematic Review of Reported Cases
- PMID: 30755846
- PMCID: PMC6367194
- DOI: 10.7150/jbji.31843
Brodie's Abscess: A Systematic Review of Reported Cases
Abstract
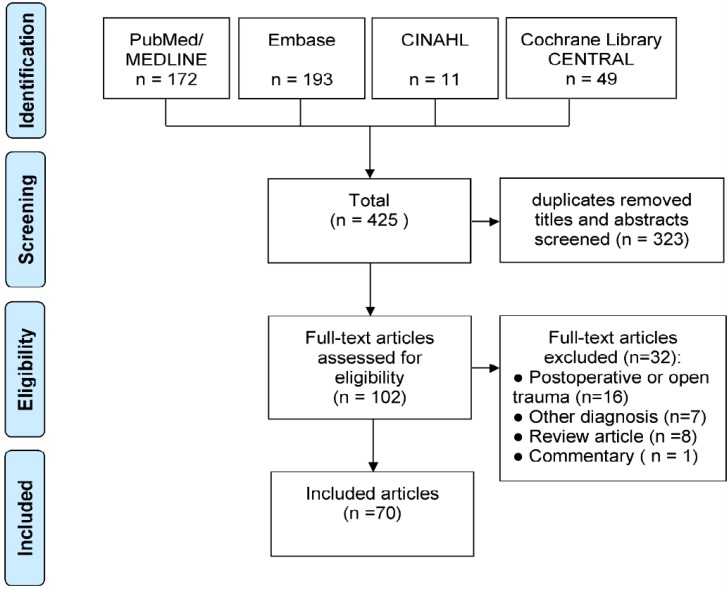
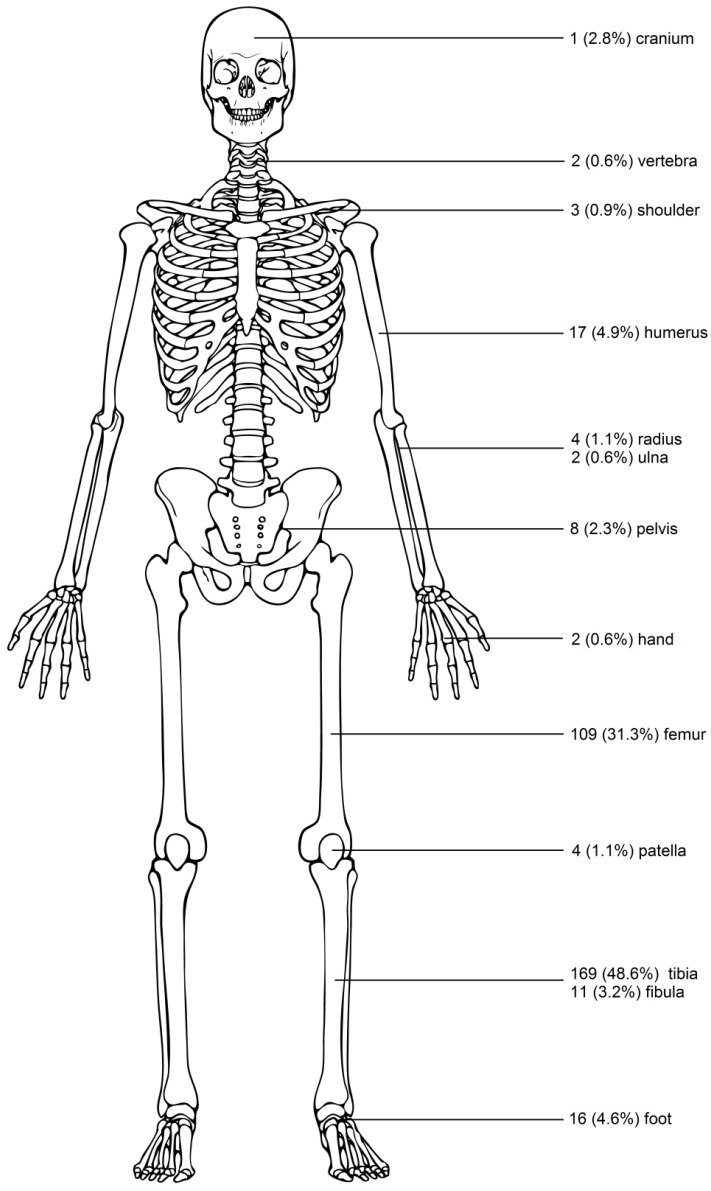
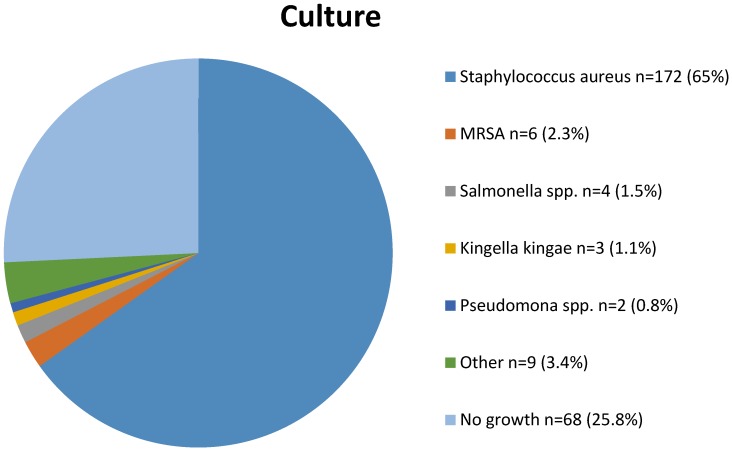
Introduction: Brodie's abscess is a form of osteomyelitis. Since its first appearance in the medical literature in 1832, numerous cases have been described. The aim of this article is to provide the first comprehensive overview of published cases of Brodie's abscess, and to describe diagnostic methods, therapeutic consequences and outcomes. Methods: According to PRISMA guidelines a systematic review of the literature was performed. All published data in English or Dutch were considered for inclusion with no limitations on publication date. Data was extracted on demography, duration of symptoms, signs of inflammation, diagnostic imaging, causative agent, treatment and follow-up. Results: A total of 70 articles were included, reporting on a total of 407 patients, mostly young (median age 17) males (male:female ratio 2.1:1). The median duration of symptoms before diagnosis was 12 weeks (SD 26). Mostly consisting of pain (98%) and/or swelling (53%). 84% of all patients were afebrile, and less than 50% had elevated serum inflammation markers. Diagnosis was made with a combination of imaging modalities: plain X-ray in 96%, MRI (16%) and CT-scan (8%). Treatment consisted of surgery in 94% of the cases, in conjunction with long term antibiotics in 77%. Staphylococcus aureus was the pathogen most often found in the culture (67,3%). Outcome was generally reported as favorable. Recurrence was reported in 15,6% of the cases requiring further intervention. Two cases developed permanent disability. Conclusion: Brodie's abscess has an insidious onset as systemic inflammatory signs and symptoms were often not found. Treatment consisted mostly of surgery followed by antibiotics (77%) or only surgery (17%) and outcomes were generally reported as favourable.
Keywords: Brodie's abscess; case report; osteomyelitis; systematic review.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
References
-
- Harris NH, Kirkaldy WH. Primary Subacute Pyogenic osteomyelitis. J Bone Joint Surg Br. England. 1965 Aug;47:526–32. - PubMed
-
- Metsemakers WJ, Morgenstern M, McNally MA, Moriarty TF, McFadyen I, Scarborough M. et al. Fracture-related infection: A consensus on definition from an international expert group. Injury. Netherlands. 2018 Mar;49(3):505–10. - PubMed
-
- Lew DP, Waldvogel FA. Osteomyelitis. Lancet; 2004. pp. 369–79. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
