

Relapse prevention interventions for smoking cessation
- PMID: 30758045
- PMCID: PMC6372978
- DOI: 10.1002/14651858.CD003999.pub5
Relapse prevention interventions for smoking cessation
Update in
-
Relapse prevention interventions for smoking cessation.Cochrane Database Syst Rev. 2019 Oct 28;2019(10):CD003999. doi: 10.1002/14651858.CD003999.pub6. Cochrane Database Syst Rev. 2019. PMID: 31684681 Free PMC article.
Abstract
Background: A number of treatments can help smokers make a successful quit attempt, but many initially successful quitters relapse over time. Several interventions have been proposed to help prevent relapse.
Objectives: To assess whether specific interventions for relapse prevention reduce the proportion of recent quitters who return to smoking.
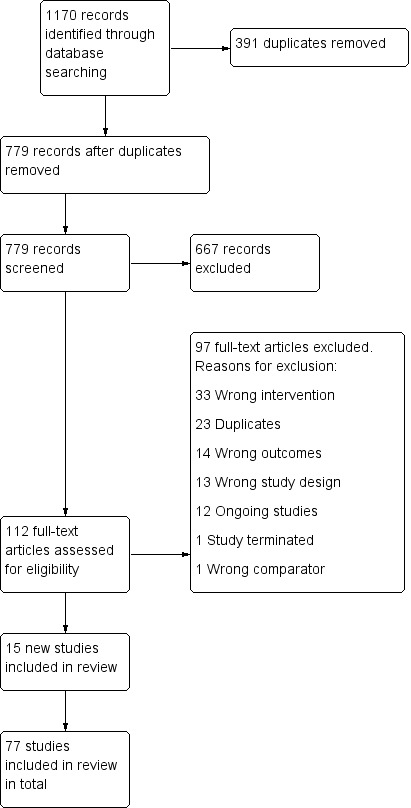
Search methods: We searched the Cochrane Tobacco Addiction Group trials register, clinicaltrials.gov, and the ICTRP in February 2018 for studies mentioning relapse prevention or maintenance in their title, abstracts, or keywords.
Selection criteria: Randomised or quasi-randomised controlled trials of relapse prevention interventions with a minimum follow-up of six months. We included smokers who quit on their own, were undergoing enforced abstinence, or were participating in treatment programmes. We included studies that compared relapse prevention interventions with a no intervention control, or that compared a cessation programme with additional relapse prevention components with a cessation programme alone.
Data collection and analysis: We used standard methodological procedures expected by Cochrane.
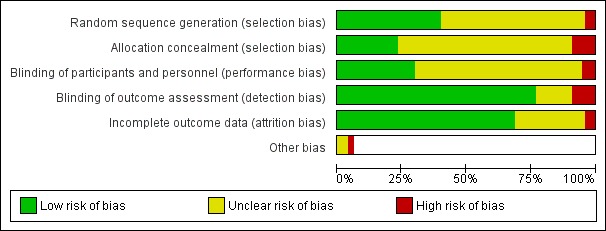
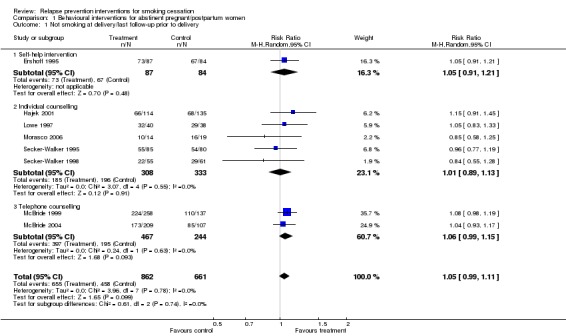
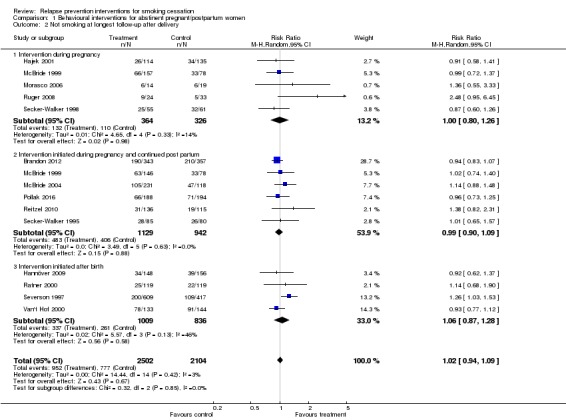
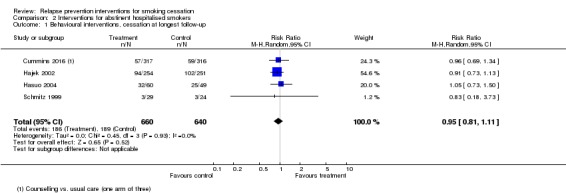
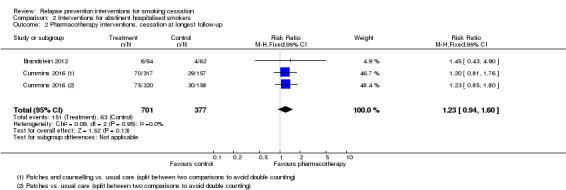
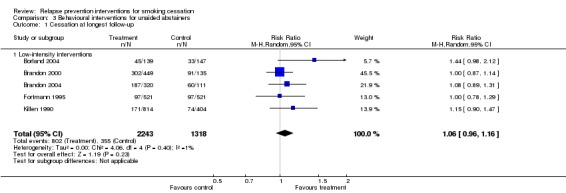
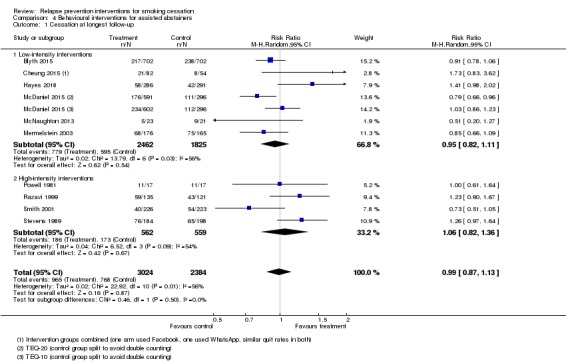
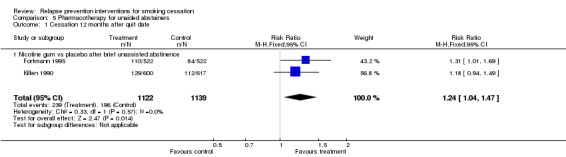
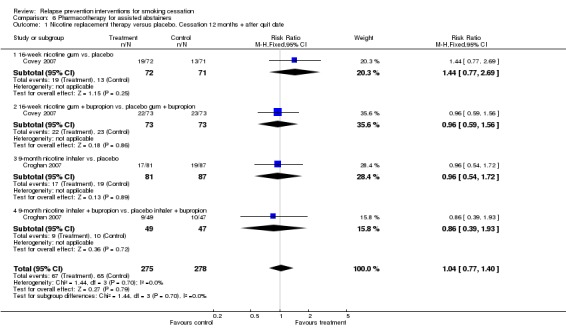
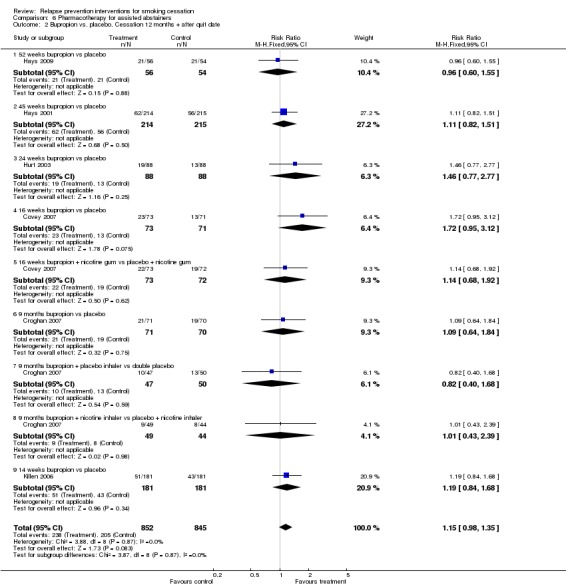
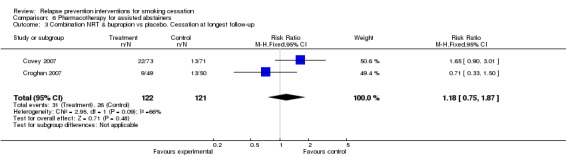
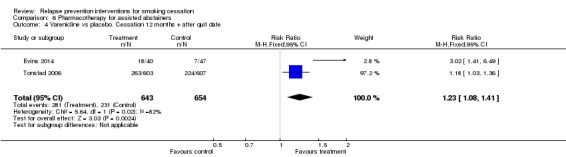
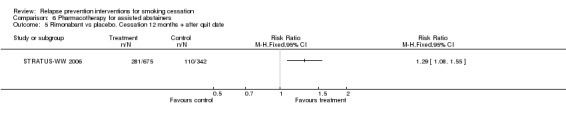
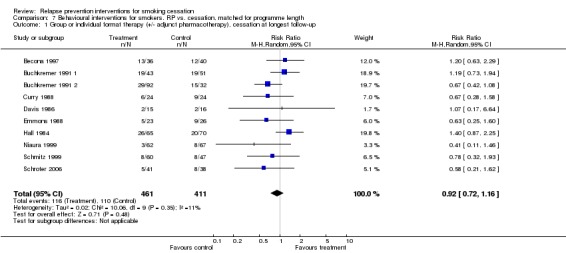
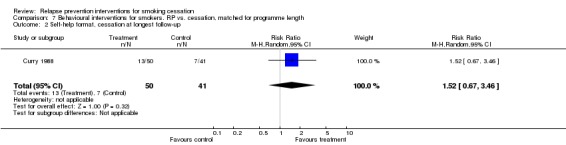
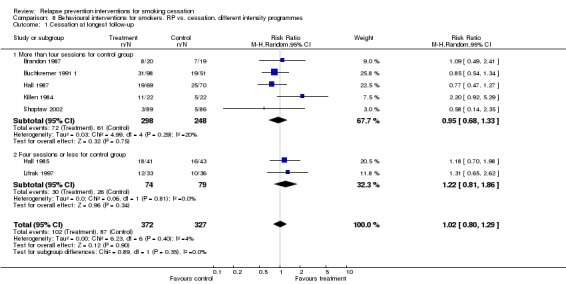
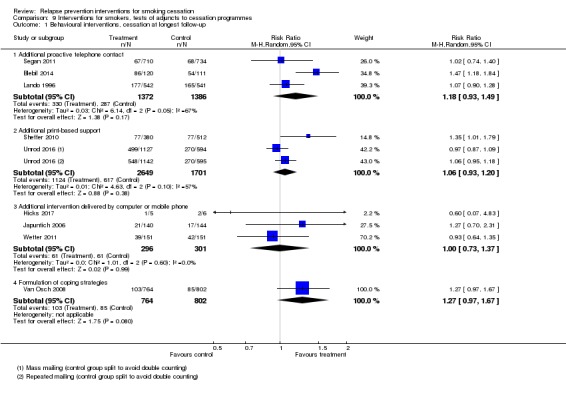
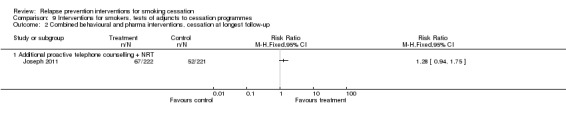
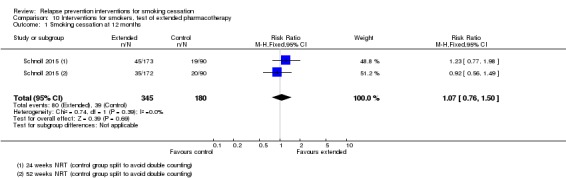
Main results: We included 77 studies (67,285 participants), 15 of which are new to this update. We judged 21 studies to be at high risk of bias, 51 to be at unclear risk of bias, and five studies to be at low risk of bias. Forty-eight studies included abstainers, and 29 studies helped people to quit and then tested treatments to prevent relapse. Twenty-six studies focused on special populations who were abstinent because of pregnancy (18 studies), hospital admission (five studies), or military service (three studies). Most studies used behavioural interventions that tried to teach people skills to cope with the urge to smoke, or followed up with additional support. Some studies tested extended pharmacotherapy.We focused on results from those studies that randomised abstainers, as these are the best test of relapse prevention interventions. Of the 12 analyses we conducted in abstainers, three pharmacotherapy analyses showed benefits of the intervention: extended varenicline in assisted abstainers (2 studies, n = 1297, risk ratio (RR) 1.23, 95% confidence interval (CI) 1.08 to 1.41, I² = 82%; moderate certainty evidence), rimonabant in assisted abstainers (1 study, RR 1.29, 95% CI 1.08 to 1.55), and nicotine replacement therapy (NRT) in unaided abstainers (2 studies, n = 2261, RR 1.24, 95% Cl 1.04 to 1.47, I² = 56%). The remainder of analyses of pharmacotherapies in abstainers had wide confidence intervals consistent with both no effect and a statistically significant effect in favour of the intervention. These included NRT in hospital inpatients (2 studies, n = 1078, RR 1.23, 95% CI 0.94 to 1.60, I² = 0%), NRT in assisted abstainers (2 studies, n = 553, RR 1.04, 95% CI 0.77 to 1.40, I² = 0%; low certainty evidence), extended bupropion in assisted abstainers (6 studies, n = 1697, RR 1.15, 95% CI 0.98 to 1.35, I² = 0%; moderate certainty evidence), and bupropion plus NRT (2 studies, n = 243, RR 1.18, 95% CI 0.75 to 1.87, I² = 66%; low certainty evidence). Analyses of behavioural interventions in abstainers did not detect an effect. These included studies in abstinent pregnant and postpartum women at end of pregnancy (8 studies, n = 1523, RR 1.05, 95% CI 0.99 to 1.11, I² = 0%) and at postpartum follow-up (15 studies, n = 4606, RR 1.02, 95% CI 0.94 to 1.09, I² = 3%), studies in hospital inpatients (4 studies, n = 1300, RR 0.95, 95% CI 0.81 to 1.11, I² = 0%), and studies in assisted abstainers (10 studies, n = 5408, RR 0.99, 95% CI 0.87 to 1.13, I² = 56%; moderate certainty evidence) and unaided abstainers (5 studies, n = 3561, RR 1.06, 95% CI 0.96 to 1.16, I² = 1%) from the general population.
Authors' conclusions: Behavioural interventions that teach people to recognise situations that are high risk for relapse along with strategies to cope with them provided no worthwhile benefit in preventing relapse in assisted abstainers, although unexplained statistical heterogeneity means we are only moderately certain of this. In people who have successfully quit smoking using pharmacotherapy, there were mixed results regarding extending pharmacotherapy for longer than is standard. Extended treatment with varenicline helped to prevent relapse; evidence for the effect estimate was of moderate certainty, limited by unexplained statistical heterogeneity. Moderate-certainty evidence, limited by imprecision, did not detect a benefit from extended treatment with bupropion, though confidence intervals mean we could not rule out a clinically important benefit at this stage. Low-certainty evidence, limited by imprecision, did not show a benefit of extended treatment with nicotine replacement therapy in preventing relapse in assisted abstainers. More research is needed in this area, especially as the evidence for extended nicotine replacement therapy in unassisted abstainers did suggest a benefit.
Conflict of interest statement
JLB: none known
EN: none known
JHB: none known
RW has received payments for lectures, research and consultancy from companies that manufacture smoking cessation medications (Pfizer, GSK, J&J). He is an unpaid advisor on the Smoke Free smartphone application and to the National Centre for Smoking Cessation and Training.
MJ: none known
PH was involved in three of the studies included in the review, and has provided consultancy for and received a research grant from Pfizer, a manufacturer of smoking cessation medications.
Figures

Update of
-
Relapse prevention interventions for smoking cessation.Cochrane Database Syst Rev. 2013 Aug 20;(8):CD003999. doi: 10.1002/14651858.CD003999.pub4. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2019 Feb 13;2:CD003999. doi: 10.1002/14651858.CD003999.pub5. PMID: 23963584 Updated.
References
References to studies included in this review
-
- Becona E, Vazquez FL. Does using relapse prevention increase the efficacy of a program for smoking cessation? An empirical study. Psychological Reports 1997;81(1):291‐6. - PubMed
-
- Blyth A, Maskrey V, Notley C, Barton GR, Brown TJ, Aveyard P, et al. Effectiveness and economic evaluation of self‐help educational materials for the prevention of smoking relapse: randomised controlled trial. Health Technology Assessment 2015;19(59):1‐70. - PMC - PubMed
- Maskrey V, Blyth A, Brown TJ, Barton GR, Notley C, Aveyard P, et al. Self‐help educational booklets for the prevention of smoking relapse following smoking cessation treatment: a randomized controlled trial. Addiction 2015;110(12):No Pagination Specified. - PMC - PubMed
- Song F, Holland R, Barton GR, Bachmann M, Blyth A, Maskrey V, et al. Self‐help materials for the prevention of smoking relapse: study protocol for a randomized controlled trial. Trials 2012;13:69. - PMC - PubMed
-
- Borland R, Balmford J, Hunt D. The effectiveness of personally tailored computer‐generated advice letters for smoking cessation. Addiction 2004;99:369‐77. - PubMed
-
- Brandon TH, Zelman DC, Baker TB. Effects of maintenance sessions on smoking relapse: delaying the inevitable?. Journal of Consulting and Clinical Psychology 1987;55:780‐2. - PubMed
References to studies excluded from this review
-
- Adams KK, Merritt TA. Prevention of postpartum smoking relapse in mothers to prevent infant exposure to second‐hand smoke. Journal of Investigative Medicine 2011;59:102.
-
- Allen S, Bade T, Hatsukami D. Smoking relapse in women: effect of menstrual phase. SYM 10B Society for Research on Nicotine and Tobacco 13th Annual Meeting; 2007 February 21‐24; Austin, TX. 2007.
-
- Alterman AI, Gariti P, Mulvaney F. Short‐ and long‐term smoking cessation for three levels of intensity of behavioral treatment. Psychology of Addictive Behaviors 2001;15(3):261‐4. - PubMed
-
- Bottausci AJ. An experimental study of cue exposure as a relapse prevention technique in smoking cessation maintenance. Masters Abstracts International 1995;32(3):1063.
References to ongoing studies
-
- Brandon TH, Klesges RC, Ebbert JO, Talcott GW, Thomas F, Leroy K, et al. Preventing smoking initiation or relapse following 8.5 weeks of involuntary smoking abstinence in basic military training: trial design, interventions, and baseline data. Contemporary Clinical Trials2014; Vol. 38, issue 1:28‐36. - PMC - PubMed
-
- Fallgatter AJ, Dieler A, Herrmann MJ, Dresler T. Non‐invasive brain stimulation ‐ a modern approach to improved therapy of nicotin addiction?. Brain Stimulation 2015;8(2):429.
-
- Garvey AJ, Kalman D, Hoskinson RA, Kinnunen T, Armour CD, Copp S, et al. Effects of extended‐duration counseling vs. shorter‐duration counseling after 1.5 years of follow‐up (POS4‐49). Society for Research on Nicotine and Tobacco 18th Annual Meeting March 13‐16. 2012:139.
Additional references
-
- Agboola S, McNeill A, Coleman T, Leonardi Bee J. A systematic review of the effectiveness of smoking relapse prevention interventions for abstinent smokers. Addiction 2010;105(8):1362‐80. - PubMed
-
- Coleman T, Agboola S, Leonardi‐Bee J, Taylor M, McEwen A, McNeill A. Relapse prevention in UK Stop Smoking Services: current practice, systematic reviews of effectiveness and cost‐effectiveness analysis. Health Technology Assessment 2010;14(49):1‐152. - PubMed
-
- Edwards CC, Woodruff SI, Conway TL. Operation Stay Quit: preventing smoking relapse among US Navy women. American Journal of Health Behavior 1999;23(5):352‐5.
References to other published versions of this review
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical