Assessing Shoulder Biomechanics of Healthy Elderly Individuals During Activities of Daily Living Using Inertial Measurement Units: High Maximum Elevation Is Achievable but Rarely Used
- PMID: 30758509
- PMCID: PMC6434324
- DOI: 10.1115/1.4042433
Assessing Shoulder Biomechanics of Healthy Elderly Individuals During Activities of Daily Living Using Inertial Measurement Units: High Maximum Elevation Is Achievable but Rarely Used
Abstract
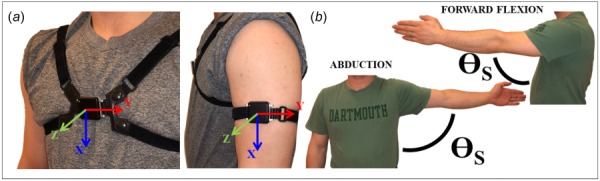
Current shoulder clinical range of motion (ROM) assessments (e.g., goniometric ROM) may not adequately represent shoulder function beyond controlled clinical settings. Relative inertial measurement unit (IMU) motion quantifies ROM precisely and can be used outside of clinic settings capturing "real-world" shoulder function. A novel IMU-based shoulder elevation quantification method was developed via IMUs affixed to the sternum/humerus, respectively. This system was then compared to in-laboratory motion capture (MOCAP) during prescribed motions (flexion, abduction, scaption, and internal/external rotation). MOCAP/IMU elevation were equivalent during flexion (R2 = 0.96, μError = 1.7 deg), abduction (R2 = 0.96, μError = 2.9 deg), scaption (R2 = 0.98, μError = -0.3 deg), and internal/external rotation (R2 = 0.90, μError = 0.4 deg). When combined across movements, MOCAP/IMU elevation were equal (R2 = 0.98, μError = 1.4 deg). Following validation, the IMU-based system was deployed prospectively capturing continuous shoulder elevation in 10 healthy individuals (4 M, 69 ± 20 years) without shoulder pathology for seven consecutive days (13.5 ± 2.9 h/day). Elevation was calculated continuously daily and outcome metrics included percent spent in discrete ROM (e.g., 0-5 deg and 5-10 deg), repeated maximum elevation (i.e., >10 occurrences), and maximum/average elevation. Average elevation was 40 ± 6 deg. Maximum with >10 occurrences and maximum were on average 145-150 deg and 169 ± 8 deg, respectively. Subjects spent the vast majority of the day (97%) below 90 deg of elevation, with the most time spent in the 25-30 deg range (9.7%). This study demonstrates that individuals have the ability to achieve large ROMs but do not frequently do so. These results are consistent with the previously established lab-based measures. Moreover, they further inform how healthy individuals utilize their shoulders and may provide clinicians a reference for postsurgical ROM.
Figures






Similar articles
-
Continuously monitoring shoulder motion after total shoulder arthroplasty: maximum elevation and time spent above 90° of elevation are critical metrics to monitor.J Shoulder Elbow Surg. 2019 Aug;28(8):1505-1514. doi: 10.1016/j.jse.2019.01.003. Epub 2019 Apr 5. J Shoulder Elbow Surg. 2019. PMID: 30956145 Free PMC article.
-
Development of a 3D workspace shoulder assessment tool incorporating electromyography and an inertial measurement unit-a preliminary study.Med Biol Eng Comput. 2018 Jun;56(6):1003-1011. doi: 10.1007/s11517-017-1745-4. Epub 2017 Nov 11. Med Biol Eng Comput. 2018. PMID: 29127653 Free PMC article.
-
Assessment of Shoulder Range of Motion Using a Wireless Inertial Motion Capture Device-A Validation Study.Sensors (Basel). 2019 Apr 13;19(8):1781. doi: 10.3390/s19081781. Sensors (Basel). 2019. PMID: 31013931 Free PMC article.
-
Quantifying shoulder motion in the free-living environment using wearable inertial measurement units: Challenges and recommendations.J Biomech. 2025 Mar;182:112589. doi: 10.1016/j.jbiomech.2025.112589. Epub 2025 Feb 17. J Biomech. 2025. PMID: 39987887 Review.
-
Concurrent validity of inertial measurement units in range of motion measurements of upper extremity: A systematic review and meta-analysis.Wearable Technol. 2024 Oct 4;5:e11. doi: 10.1017/wtc.2024.6. eCollection 2024. Wearable Technol. 2024. PMID: 39464639 Free PMC article. Review.
Cited by
-
Clinical outcomes and complications of reverse shoulder arthroplasty used for failed prior shoulder surgery: a systematic review and meta-analysis.JSES Int. 2020 Jan 3;4(1):156-168. doi: 10.1016/j.jses.2019.10.108. eCollection 2020 Mar. JSES Int. 2020. PMID: 32195479 Free PMC article. Review.
-
Prediction of Lower Limb Kinetics and Kinematics during Walking by a Single IMU on the Lower Back Using Machine Learning.Sensors (Basel). 2019 Dec 24;20(1):130. doi: 10.3390/s20010130. Sensors (Basel). 2019. PMID: 31878224 Free PMC article.
-
Measuring 3D In-vivo Shoulder Kinematics using Biplanar Videoradiography.J Vis Exp. 2021 Mar 12;(169):10.3791/62210. doi: 10.3791/62210. J Vis Exp. 2021. PMID: 33779606 Free PMC article.
-
Monitoring Scapular Kinematics through Wearable Magneto-Inertial Measurement Units: State of the Art and New Frontiers.Sensors (Basel). 2023 Aug 4;23(15):6940. doi: 10.3390/s23156940. Sensors (Basel). 2023. PMID: 37571723 Free PMC article.
-
Changes in shoulder range of motion following arthroscopic rotator cuff repair: a systematic review.BMC Musculoskelet Disord. 2025 Jul 4;26(1):600. doi: 10.1186/s12891-025-08579-y. BMC Musculoskelet Disord. 2025. PMID: 40615794 Free PMC article.
References
-
- Ilfeld, B. M. , Wright, T. W. , Enneking, F. K. , and Morey, T. E. , 2005, “Joint Range of Motion After Total Shoulder Arthroplasty With and Without a Continuous Interscalene Nerve Block: A Retrospective, Case-Control Study,” Reg. Anesth. Pain Med., 30(5), pp. 429–433.10.1016/j.rapm.2005.06.003 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous