

A case of successfully resected metachronous gastric and gallbladder metastases from pancreatic body cancer
- PMID: 30758733
- PMCID: PMC6374494
- DOI: 10.1186/s40792-019-0581-1
A case of successfully resected metachronous gastric and gallbladder metastases from pancreatic body cancer
Abstract
Background: Pancreatic ductal adenocarcinoma (PDAC) readily metastasizes to the lymph nodes, liver, lung, and peritoneum; however, gastric and gallbladder metastases are rare. We report a case of metachronous gastric and gallbladder metastases from PDAC.
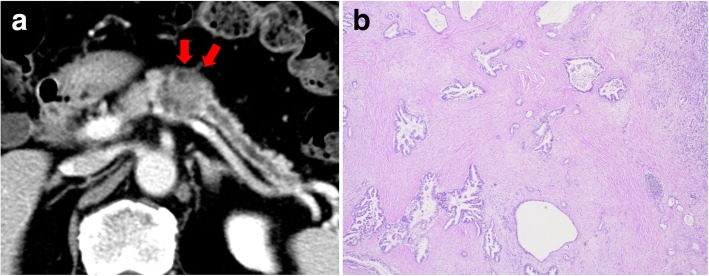
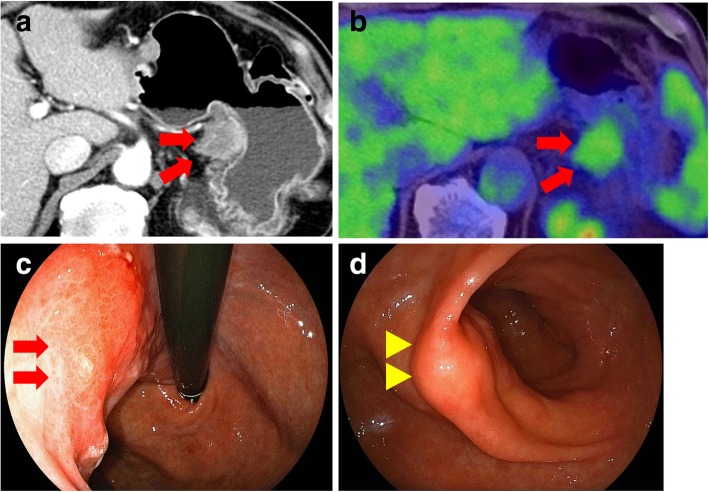
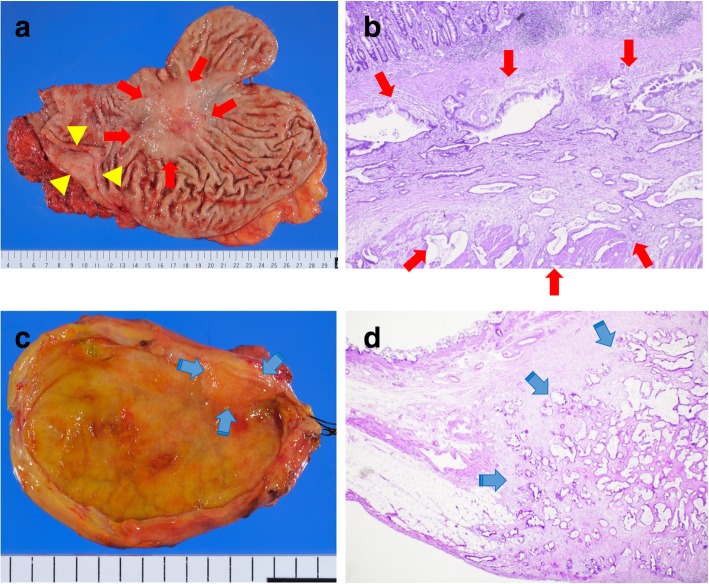
Case presentation: The patient is a 71-year-old man who underwent distal pancreatectomy for PDAC. Seventeen months after the surgery, a 30-mm nodule was detected at the lesser curvature of the stomach, which was diagnosed as recurrence of PDAC in the lymph nodes. He then received gemcitabine and S-1 combination chemotherapy for 6 months. Because tumor size remained approximately the same and tumor marker levels decreased, total gastrectomy and cholecystectomy were performed. Pathological examination showed well-differentiated tubular adenocarcinoma in the subserosa and muscularis propria of the stomach and gallbladder. The patient remains alive at 41 months after the second surgery with liver metastasis.
Conclusion: We reported a rare case of metachronous gastric and gallbladder metastases from pancreatic body cancer.
Keywords: Metachronous gallbladder metastasis; Metachronous gastric metastasis; Pancreatic cancer; Surgery.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Informed consent was obtained from the patient for the publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Long-term survival after hepatectomy for metachronous liver metastasis of pancreatic ductal adenocarcinoma: a case report.Surg Case Rep. 2020 Jul 3;6(1):157. doi: 10.1186/s40792-020-00924-8. Surg Case Rep. 2020. PMID: 32621095 Free PMC article.
-
[A Case of Synchronous and Solitary Gallbladder Metastasis from Gastric Cancer].Gan To Kagaku Ryoho. 2019 Nov;46(11):1765-1769. Gan To Kagaku Ryoho. 2019. PMID: 31748489 Review. Japanese.
-
Triple metachronous primary pancreatic and gallbladder cancer associated with pancreaticobiliary maljunction: a case report.Surg Case Rep. 2021 Apr 6;7(1):81. doi: 10.1186/s40792-021-01160-4. Surg Case Rep. 2021. PMID: 33825072 Free PMC article.
-
Simultaneous brain and lung metastases of pancreatic ductal adenocarcinoma after curative pancreatectomy: a case report and literature review.BMC Gastroenterol. 2021 Jan 6;21(1):9. doi: 10.1186/s12876-020-01587-3. BMC Gastroenterol. 2021. PMID: 33407200 Free PMC article. Review.
-
[A case of metachronous pancreatic cancer that developed 4 years after initial pancreatectomy].Gan To Kagaku Ryoho. 2013 Nov;40(12):1893-6. Gan To Kagaku Ryoho. 2013. PMID: 24393957 Review. Japanese.
Cited by
-
Synchronous concomitant pancreatic acinar cell carcin and gastric adenocarcinoma: A case report and review of literature.World J Clin Cases. 2021 Oct 6;9(28):8509-8517. doi: 10.12998/wjcc.v9.i28.8509. World J Clin Cases. 2021. PMID: 34754861 Free PMC article.
-
Long-Term Survival after Curative Resection for Postoperative Dissemination of Pancreatic Ductal Adenocarcinoma: A Case Report.Surg Case Rep. 2025;11(1):24-0022. doi: 10.70352/scrj.cr.24-0022. Epub 2025 Apr 2. Surg Case Rep. 2025. PMID: 40196210 Free PMC article.
-
Multiple Gastric Metastases after Distal Pancreatectomy for Pancreatic Cancer.Intern Med. 2022 Sep 15;61(18):2741-2746. doi: 10.2169/internalmedicine.8848-21. Epub 2022 Feb 26. Intern Med. 2022. PMID: 35228419 Free PMC article.
-
Intraduodenal wall recurrence 11 years after distal pancreatectomy for pancreatic ductal adenocarcinoma.Clin J Gastroenterol. 2025 Aug;18(4):695-699. doi: 10.1007/s12328-025-02141-y. Epub 2025 May 16. Clin J Gastroenterol. 2025. PMID: 40377880 Free PMC article.
-
Curative resection after chemotherapy and chemoradiotherapy for postoperative recurrence of pancreatic tail cancer in the abdominal wall: a case report.Surg Case Rep. 2022 May 19;8(1):101. doi: 10.1186/s40792-022-01452-3. Surg Case Rep. 2022. PMID: 35585274 Free PMC article.
References
-
- Ueno H, Ioka T, Ikeda M, Ohkawa S, Yanagimoto H, Boku N, et al. Randomized phase III study of gemcitabine plus S-1, S-1 alone, or gemcitabine alone in patients with locally advanced and metastatic pancreatic cancer in Japan and Taiwan: GEST study. J Clini Oncol. 2013;31(13):1640–1648. doi: 10.1200/JCO.2012.43.3680. - DOI - PubMed
LinkOut - more resources
Full Text Sources
