

Disease trajectories in childhood atopic dermatitis: an update and practitioner's guide
- PMID: 30758843
- PMCID: PMC6899789
- DOI: 10.1111/bjd.17766
Disease trajectories in childhood atopic dermatitis: an update and practitioner's guide
Abstract
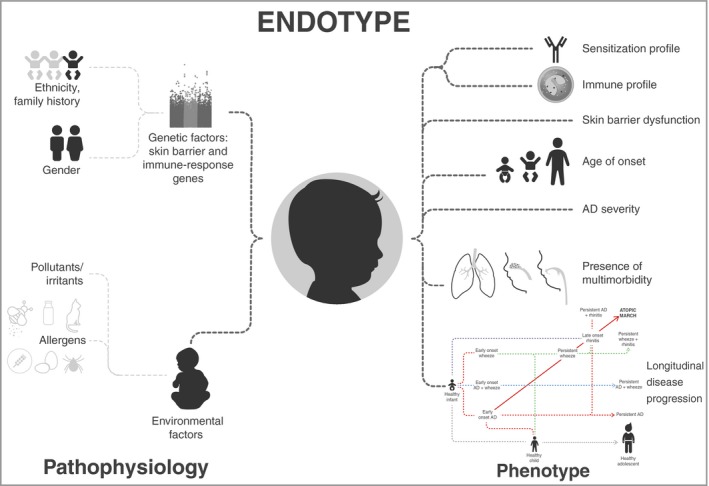
Background: Atopic dermatitis (AD) is a heterogeneous disease with a multifactorial aetiology and complex pathophysiology. This heterogeneity translates into different trajectories of disease progression with respect to severity, persistence and risk of development of atopic comorbidities. Determining which possible disease trajectories or comorbidities any individual child might develop is challenging in clinical practice. Tools that help identify paediatric patients at higher risk of disease progression would greatly aid clinicians.
Methods: We reviewed recent cohort studies to synthesize and simplify the epidemiological data to try to identify shared clinically relevant characteristics that may help physicians estimate the risk of disease progression in paediatric patients with AD.
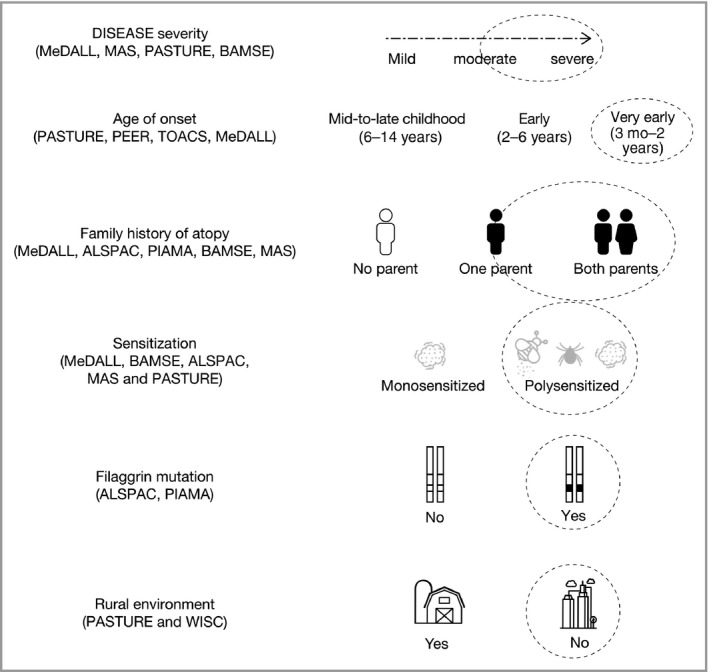
Results: Despite the variability in data collection and methods of analysis and their limitations, there are common patterns of early-childhood AD that may aid in the estimation of risk for disease progression. Factors associated with risk of AD progression include younger age of onset, family history of atopy, greater AD severity, filaggrin mutations, urban environment and polysensitization and/or allergic multimorbidity. Based on these factors, we provide a practitioner's guide for identifying, counselling and/or referring infants and children with AD at potentially higher risk of developing persistent AD and atopic comorbidities. We also present clinical scenarios to illustrate how these data relate to real-life situations.
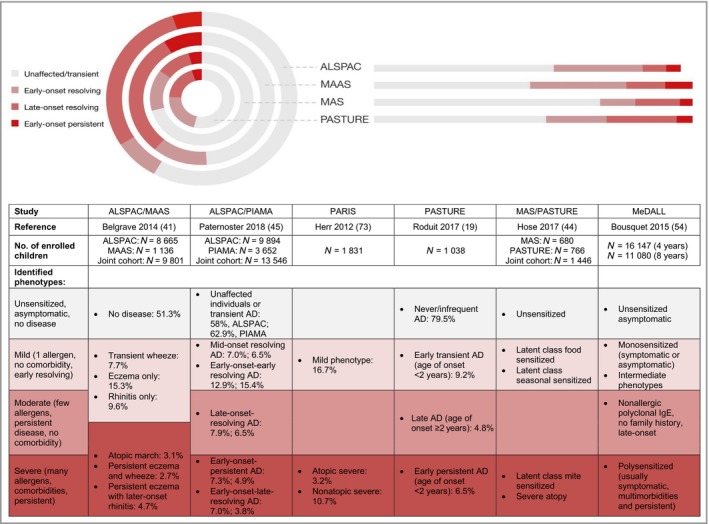
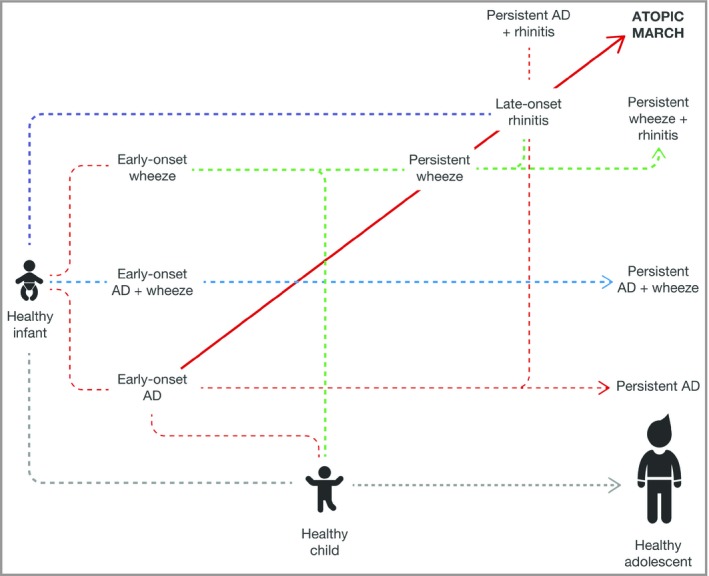
Conclusions: Useful insights are provided for physicians and patients to inform them better about the risk of AD progression and to help guide care pathways for the paediatric population with AD. What's already known about this topic? The complex pathophysiology of atopic dermatitis (AD) translates into a heterogeneous clinical presentation and trajectories of disease progression. Although the consensus is that most paediatric patients with AD will eventually 'outgrow' the disease or follow the longitudinal trajectory known as the 'atopic march', a significant proportion will develop persistent AD and/or other atopic conditions. No known factors conclusively predict the risk of progression or development of comorbidities. What does this study add? Recent analyses of data from large cohorts of paediatric patients with AD have suggested the existence of potentially discrete clusters of patients who present with relatively common AD phenotypes. These studies have shed some light onto the factors associated with risk of progression, which we review in this article. A practitioner's guide with clinical scenarios is provided to help identify patients at high risk of progression to determine whether a patient should be monitored and/or would require specialist referral.
© 2019 The Authors. British Journal of Dermatology published by John Wiley & Sons Ltd on behalf of British Association of Dermatologists.
Figures
Comment in
-
Atopic dermatitis epidemiology: moving beyond cross-sectional studies.Br J Dermatol. 2019 Nov;181(5):883-884. doi: 10.1111/bjd.18440. Epub 2019 Sep 8. Br J Dermatol. 2019. PMID: 31494927 No abstract available.
Similar articles
-
Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis.J Am Acad Dermatol. 2014 Feb;70(2):338-51. doi: 10.1016/j.jaad.2013.10.010. Epub 2013 Nov 27. J Am Acad Dermatol. 2014. PMID: 24290431 Free PMC article. Review.
-
Genetic, Clinical, and Environmental Factors Associated With Persistent Atopic Dermatitis in Childhood.JAMA Dermatol. 2019 Jan 1;155(1):50-57. doi: 10.1001/jamadermatol.2018.4061. JAMA Dermatol. 2019. PMID: 30427975 Free PMC article.
-
Different definitions of atopic dermatitis: impact on prevalence estimates and associated risk factors.Br J Dermatol. 2019 Dec;181(6):1272-1279. doi: 10.1111/bjd.17853. Epub 2019 Jun 26. Br J Dermatol. 2019. PMID: 30822368 Free PMC article. Review.
-
Clinical Characteristics of Atopic Dermatitis in Korean School-Aged Children and Adolescents According to Onset Age and Severity.J Korean Med Sci. 2022 Jan 24;37(4):e30. doi: 10.3346/jkms.2022.37.e30. J Korean Med Sci. 2022. PMID: 35075829 Free PMC article.
-
Risk factors and temporal associations of progression of the atopic march in children with early-onset atopic dermatitis.J Am Acad Dermatol. 2025 Apr;92(4):732-740. doi: 10.1016/j.jaad.2024.10.107. Epub 2024 Nov 28. J Am Acad Dermatol. 2025. PMID: 39615548
Cited by
-
The Role of the Environment and Exposome in Atopic Dermatitis.Curr Treat Options Allergy. 2021;8(3):222-241. doi: 10.1007/s40521-021-00289-9. Epub 2021 May 21. Curr Treat Options Allergy. 2021. PMID: 34055570 Free PMC article. Review.
-
Topical corticosteroids normalize both skin and systemic inflammatory markers in infant atopic dermatitis.Br J Dermatol. 2021 Jul;185(1):153-163. doi: 10.1111/bjd.19703. Epub 2021 Mar 7. Br J Dermatol. 2021. PMID: 33269467 Free PMC article.
-
Evaluation of dupilumab on the disease burden in children and adolescents with atopic dermatitis: A population-based cohort study.Allergy. 2024 Oct;79(10):2748-2758. doi: 10.1111/all.16265. Epub 2024 Aug 21. Allergy. 2024. PMID: 39166365
-
Dupilumab Efficacy in Children with Atopic Dermatitis with Different Phenotypes and Endotypes: A Case Series.Adv Ther. 2025 Jul;42(7):3186-3206. doi: 10.1007/s12325-025-03150-6. Epub 2025 May 8. Adv Ther. 2025. PMID: 40338484 Free PMC article. Clinical Trial.
-
Atopic dermatitis trajectories to age 8 years in the GUSTO cohort.Clin Exp Allergy. 2021 Sep;51(9):1195-1206. doi: 10.1111/cea.13993. Epub 2021 Jul 31. Clin Exp Allergy. 2021. PMID: 34310791 Free PMC article.
References
-
- Garg N, Silverberg JI. Epidemiology of childhood atopic dermatitis. Clin Dermatol 2015; 33:281–8. - PubMed
-
- Spergel JM. Epidemiology of atopic dermatitis and atopic march in children. Immunol Allergy Clin North Am 2010; 30:269–80. - PubMed
-
- Weidinger S, Novak N. Atopic dermatitis. Lancet 2016; 387:1109–22. - PubMed
-
- Guttman‐Yassky E, Waldman A, Ahluwalia J et al Atopic dermatitis: pathogenesis. Semin Cutan Med Surg 2017; 36:100–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
