

Improving Detection of Early Chronic Obstructive Pulmonary Disease
- PMID: 30759006
- PMCID: PMC6322002
- DOI: 10.1513/AnnalsATS.201808-529MG
Improving Detection of Early Chronic Obstructive Pulmonary Disease
Abstract
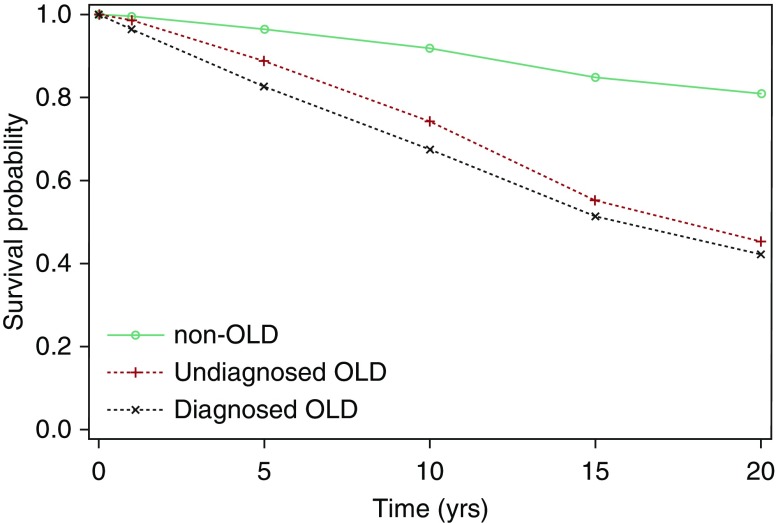
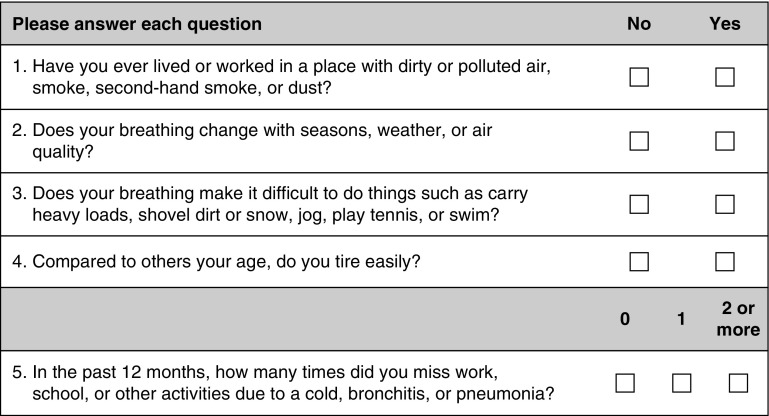
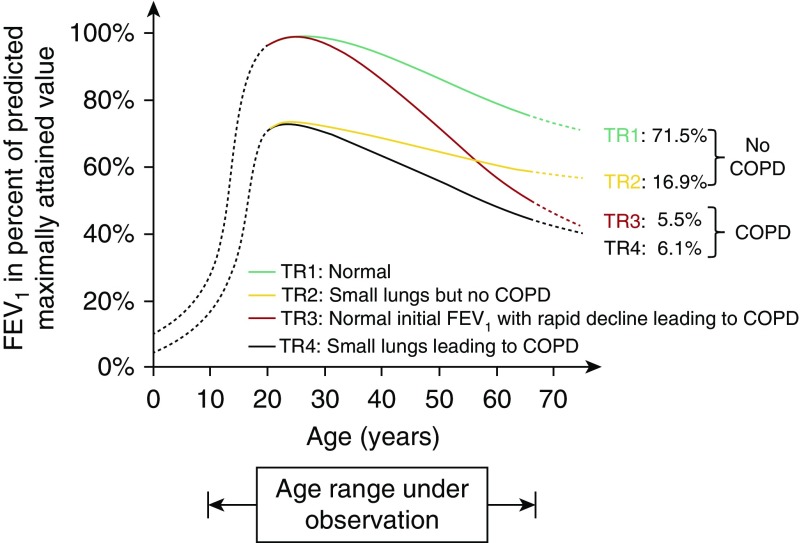
Despite being a major cause of morbidity and mortality, chronic obstructive pulmonary disease (COPD) is frequently undiagnosed. Yet the burden of disease among the undiagnosed is significant, as these individuals experience symptoms, exacerbations, and excess mortality compared to those without COPD. The U.S. Preventive Services Task Force recommends against routine screening of asymptomatic individuals with spirometry. Hence, case-finding approaches are needed. A recently developed instrument, the five-item COPD Assessment in Primary Care to Identify Undiagnosed Respiratory Disease and Exacerbation Risk questionnaire plus peak expiratory flow, demonstrates good sensitivity and specificity for distinguishing cases from control subjects and is being studied prospectively in primary care settings to determine its impact on patient outcomes. However, finding the undiagnosed is only half the battle. Mounting evidence suggests significant COPD-like respiratory burden among individuals without airflow obstruction. Many experience dyspnea, mucus production, and exacerbation events and have emphysema and airway abnormalities on computed tomographic (CT) imaging of the chest. However, it is still unclear how to best treat these individuals and which individuals go on to develop spirometric obstruction. These challenges underline the importance of defining what constitutes "early disease." A recently proposed definition characterizes early COPD as either: 1) airflow limitation, 2) compatible CT imaging abnormalities, or 3) accelerated forced expiratory volume in 1 second decline in persons younger than 50 years and with greater than a 10 pack-year smoking history. Although it is recognized that this definition does not encompass all individuals who will develop COPD, it is an attempt to identify a group of individuals with most rapid decline to better understand mechanisms of disease development and where disease-modifying interventions are most likely to be successful. Ultimately, leveraging tools such as chest CT imaging, the electronic medical record, and machine learning algorithms may aid in the identification of such individuals.
Keywords: airflow limitation; case finding; chest computed tomography; early COPD; lung function decline.
Figures
Similar articles
-
Association of pectoralis muscle area on computed tomography with airflow limitation severity and respiratory outcomes in COPD: A population-based prospective cohort study.Pulmonology. 2025 Dec 31;31(1):2416782. doi: 10.1016/j.pulmoe.2023.02.004. Epub 2024 Nov 14. Pulmonology. 2025. PMID: 36907812
-
Longitudinal Follow-Up of Participants With Tobacco Exposure and Preserved Spirometry.JAMA. 2023 Aug 1;330(5):442-453. doi: 10.1001/jama.2023.11676. JAMA. 2023. PMID: 37526720 Free PMC article.
-
Acute Exacerbations and Lung Function Loss in Smokers with and without Chronic Obstructive Pulmonary Disease.Am J Respir Crit Care Med. 2017 Feb 1;195(3):324-330. doi: 10.1164/rccm.201605-1014OC. Am J Respir Crit Care Med. 2017. PMID: 27556408 Free PMC article. Clinical Trial.
-
Chronic obstructive pulmonary disease with mild airflow limitation: current knowledge and proposal for future research - a consensus document from six scientific societies.Int J Chron Obstruct Pulmon Dis. 2017 Aug 29;12:2593-2610. doi: 10.2147/COPD.S132236. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 28919728 Free PMC article. Review.
-
Pulmonary physiology: future directions for lung function testing in COPD.Respirology. 2015 Feb;20(2):209-18. doi: 10.1111/resp.12388. Epub 2014 Sep 25. Respirology. 2015. PMID: 25257934 Review.
Cited by
-
Population reference equations for handheld peak expiratory flow in older U.S. adults.Respir Med. 2024 Nov-Dec;234:107811. doi: 10.1016/j.rmed.2024.107811. Epub 2024 Sep 19. Respir Med. 2024. PMID: 39305967
-
Implications of Managing Chronic Obstructive Pulmonary Disease in Cardiovascular Diseases.Tuberc Respir Dis (Seoul). 2021 Jan;84(1):35-45. doi: 10.4046/trd.2020.0088. Epub 2020 Oct 13. Tuberc Respir Dis (Seoul). 2021. PMID: 33045814 Free PMC article.
-
The Current Molecular and Cellular Landscape of Chronic Obstructive Pulmonary Disease (COPD): A Review of Therapies and Efforts towards Personalized Treatment.Proteomes. 2024 Aug 16;12(3):23. doi: 10.3390/proteomes12030023. Proteomes. 2024. PMID: 39189263 Free PMC article. Review.
-
Chronic respiratory diseases: a global view.Lancet Respir Med. 2020 Jun;8(6):531-533. doi: 10.1016/S2213-2600(20)30157-0. Lancet Respir Med. 2020. PMID: 32526184 Free PMC article. No abstract available.
-
A Risk Prediction Model for Mortality Among Smokers in the COPDGene® Study.Chronic Obstr Pulm Dis. 2020 Oct;7(4):346-361. doi: 10.15326/jcopdf.7.4.2020.0146. Chronic Obstr Pulm Dis. 2020. PMID: 32877963 Free PMC article.
References
-
- Brown DW, Croft JB, Greenlund KJ, Giles WH. Trends in hospitalization with chronic obstructive pulmonary disease-United States, 1990-2005. COPD. 2010;7:59–62. - PubMed
-
- Centers for Disease Control and Prevention (CDC) Deaths from chronic obstructive pulmonary disease--United States, 2000-2005. MMWR Morb Mortal Wkly Rep. 2008;57:1229–1232. - PubMed
-
- Kochanek KD, Xu J, Murphy SL, Miniño AM, Kung HC. Deaths: final data for 2009. Natl Vital Stat Rep. 2011;60:1–116. - PubMed
-
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
