

Cancer Outcomes in DCIS Patients Without Locoregional Treatment
- PMID: 30759222
- PMCID: PMC6748726
- DOI: 10.1093/jnci/djy220
Cancer Outcomes in DCIS Patients Without Locoregional Treatment
Abstract
Background: The vast majority of women diagnosed with ductal carcinoma in situ (DCIS) undergo treatment. Therefore, the risks of invasive progression and competing death in the absence of locoregional therapy are uncertain.
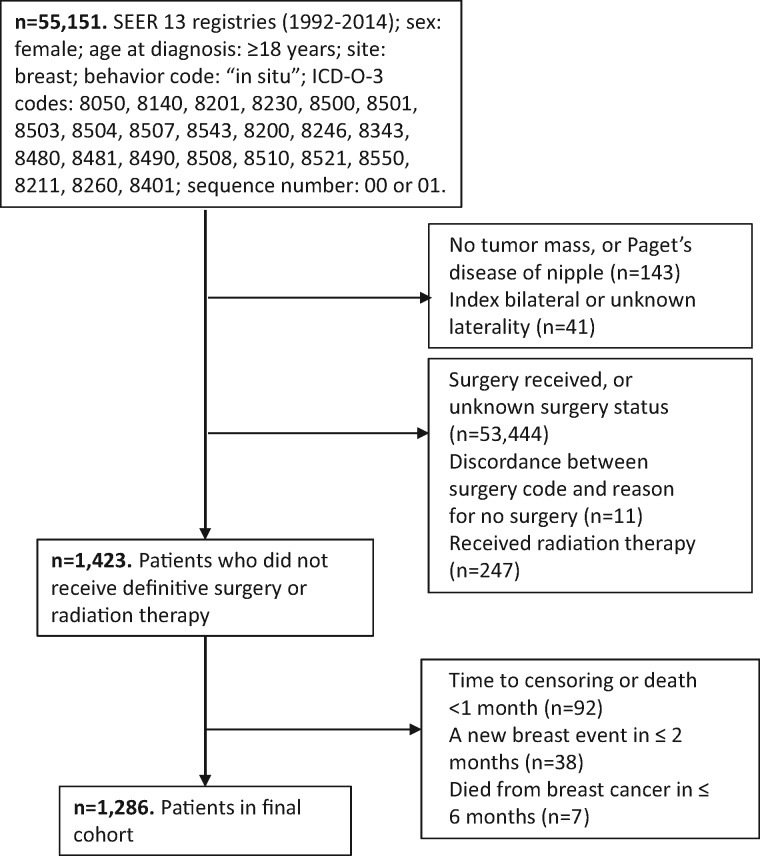
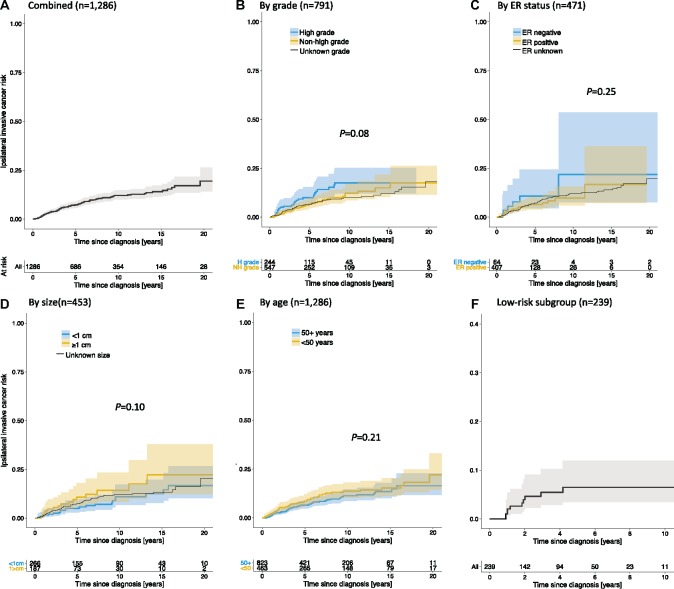
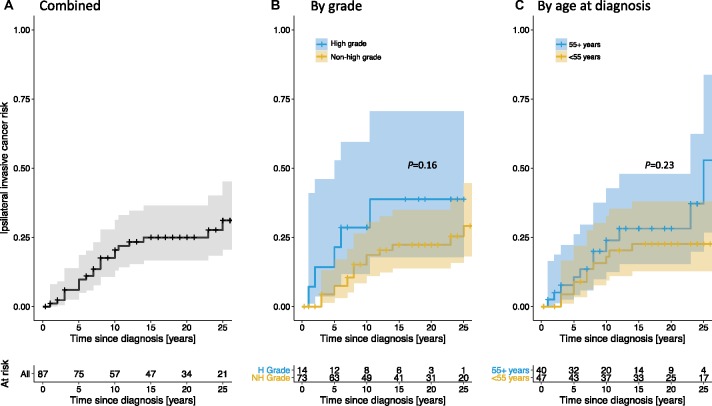
Methods: We performed survival analyses of patient-level data from DCIS patients who did not receive definitive surgery or radiation therapy as recorded in the US National Cancer Institute's Surveillance, Epidemiology, and End Results program (1992-2014). Kaplan-Meier curves were used to estimate the net risk of subsequent ipsilateral invasive cancer. The cumulative incidences of ipsilateral invasive cancer, contralateral breast cancer, and death were estimated using competing risk methods.
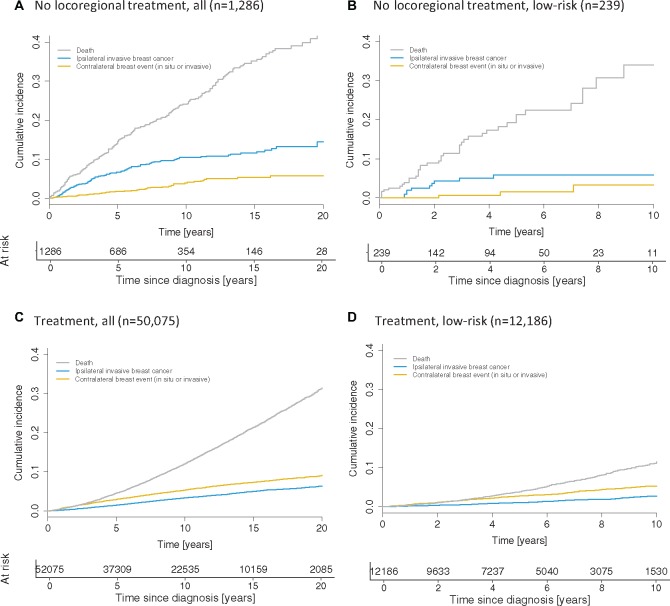
Results: A total of 1286 DCIS patients who did not undergo locoregional therapy were identified. Median age at diagnosis was 60 years (inter-quartile range = 51-74 years), with median follow-up of 5.5 years (inter-quartile range = 2.3-10.6 years). Among patients with tumor grade I/II (n = 547), the 10-year net risk of ipsilateral invasive breast cancer was 12.2% (95% confidence interval [CI] = 8.6% to 17.1%) compared with 17.6% (95% CI = 12.1% to 25.2%) among patients with tumor grade III (n = 244) and 10.1% (95% CI = 7.4% to 13.8%) among patients with unknown grade (n = 495). Among all patients, the 10-year cumulative incidences of ipsilateral invasive cancer, contralateral breast cancer, and all-cause mortality were 10.5% (95% CI = 8.5% to 12.4%), 3.9% (95% CI = 2.6% to 5.2%), and 24.1% (95% CI = 21.2% to 26.9%), respectively.
Conclusion: Despite limited data, our findings suggest that DCIS patients without locoregional treatment have a limited risk of invasive progression. Although the cohort is not representative of the general population of patients diagnosed with DCIS, the findings suggest that there may be overtreatment, especially among older patients and patients with elevated comorbidities.
© The Author(s) 2019. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Re: Cancer Outcomes in DCIS Patients Without Locoregional Treatment.J Natl Cancer Inst. 2020 Feb 1;112(2):214-215. doi: 10.1093/jnci/djz118. J Natl Cancer Inst. 2020. PMID: 31199466 Free PMC article. No abstract available.
-
Response to Habel and Buist.J Natl Cancer Inst. 2020 Feb 1;112(2):216-217. doi: 10.1093/jnci/djz120. J Natl Cancer Inst. 2020. PMID: 31199468 Free PMC article. No abstract available.
References
-
- Ward EM, DeSantis CE, Lin CC, et al. Cancer statistics: breast cancer in situ. CA Cancer J Clin. 2015;656:481–495. - PubMed
-
- Erbas B, Provenzano E, Armes J, et al. The natural history of ductal carcinoma in situ of the breast: a review. Breast Cancer Res Treat. 2006;972:135–144. - PubMed
-
- Groen EJ, Elshof LE, Visser LL, et al. Finding the balance between over- and under-treatment of ductal carcinoma in situ (DCIS). Breast. 2017;31:274–283. - PubMed
-
- Mertz BG, Duriaud HM, Kroman N, et al. Pain, sensory disturbances and psychological distress are common sequelae after treatment of ductal carcinoma in situ: a cross-sectional study. Acta Oncol. 2017;565:724–729. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
