

Early intravenous beta-blockers in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: A patient-pooled meta-analysis of randomized clinical trials
- PMID: 30759994
- PMCID: PMC7672673
- DOI: 10.1177/2048872619830609
Early intravenous beta-blockers in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: A patient-pooled meta-analysis of randomized clinical trials
Abstract
Background: Conflicting evidence is available on the efficacy and safety of early intravenous beta-blockers before primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. We performed a patient-pooled meta-analysis of trials comparing early intravenous beta-blockers with placebo or routine care in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention.
Aim: The aim of this study was to evaluate the clinical and safety outcomes of intravenous beta-blockers in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention.
Methods: Four randomized trials with a total of 1150 patients were included. The main outcome was one-year death or myocardial infarction. Secondary outcomes included biomarker-based infarct size, left ventricular ejection fraction during follow-up, ventricular tachycardia, and a composite safety outcome (cardiogenic shock, symptomatic bradycardia, or hypotension) during hospitalization.
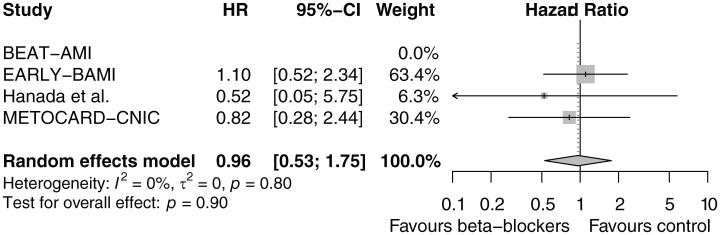
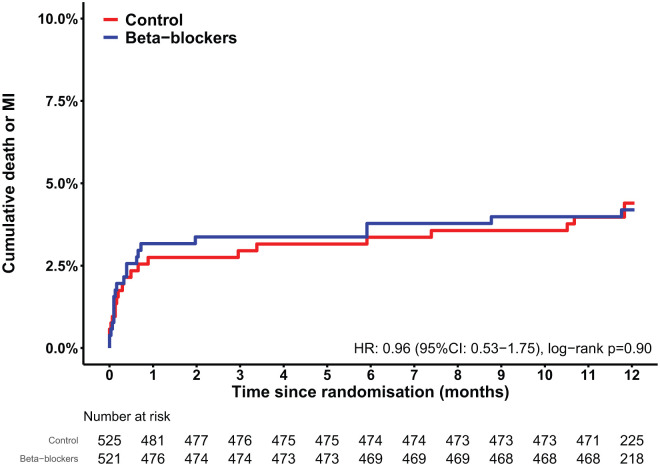
Results: One-year death or myocardial infarction was similar among beta-blocker (4.2%) and control patients (4.4%) (hazard ratio: 0.96 (95% confidence interval: 0.53-1.75, p=0.90, I2=0%). No difference was observed in biomarker-based infarct size. One-month left ventricular ejection fraction was similar, but left ventricular ejection fraction at six months was significantly higher in patients treated with early intravenous beta-blockade (52.8% versus 50.0% in the control group, p=0.03). No difference was observed in the composite safety outcome or ventricular tachycardia during hospitalization.
Conclusion: In ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention, the administration of early intravenous beta-blockers was safe. However, there was no difference in the main outcome of one-year death or myocardial infarction with early intravenous beta-blockers. A larger clinical trial is warranted to confirm the definitive efficacy of early intravenous beta-blockers.
Keywords: ST-segment elevation myocardial infarction; beta-blockers; intravenous beta-blockers; outcomes; primary percutaneous coronary intervention.
Conflict of interest statement
Figures
References
-
- Damman P, Beijk MA, Kuijt WJ, et al. Multiple biomarkers at admission significantly improve the prediction of mortality in patients undergoing primary percutaneous coronary intervention for acute ST-segment elevation myocardial infarction. J Am Coll Cardiol 2011; 57: 29–36. - PubMed
-
- Stone GW, Selker HP, Thiele H, et al. Relationship between infarct size and outcomes following primary PCI: Patient-level analysis from 10 randomized trials. J Am Coll Cardiol 2016; 67: 1674–1683. - PubMed
-
- Rasmussen MM, Reimer KA, Kloner RA, et al. Infarct size reduction by propranolol before and after coronary ligation in dogs. Circulation 1977; 56: 794–798. - PubMed
-
- Elgendy IY, Elgendy AY, Mahmoud AN, et al. Intravenous beta-blockers for patients undergoing primary percutaneous coronary intervention: A meta-analysis of randomized trials. Int J Cardiol 2016; 223: 891–897. - PubMed
-
- Er F, Dahlem KM, Nia AM, et al. Randomized control of sympathetic drive with continuous intravenous esmolol in patients with acute ST-segment elevation myocardial infarction: The BEtA-Blocker Therapy in Acute Myocardial Infarction (BEAT-AMI) Trial. JACC Cardiovasc Interv 2016; 9: 231–240. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
