

Non-Thyroidal Illness Syndrome in Critically Ill Children: Prognostic Value and Impact of Nutritional Management
- PMID: 30760183
- PMCID: PMC6457888
- DOI: 10.1089/thy.2018.0420
Non-Thyroidal Illness Syndrome in Critically Ill Children: Prognostic Value and Impact of Nutritional Management
Abstract
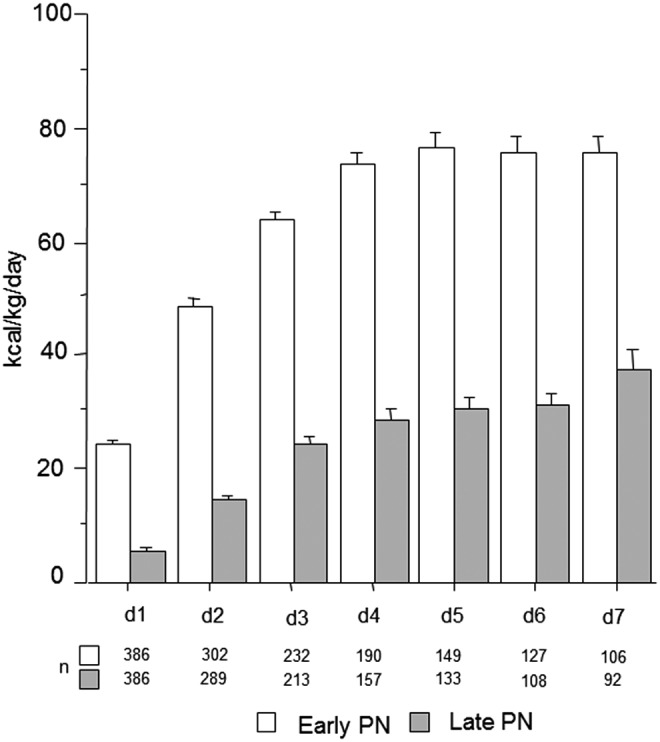
Introduction: Non-thyroidal illness (NTI), which occurs with fasting and in response to illness, is characterized by thyroid hormone inactivation with low triiodothyronine (T3) and high reverse T3 (rT3), followed by suppressed thyrotropin (TSH). Withholding supplemental parenteral nutrition early in pediatric critical illness (late-PN), thus accepting low/no macronutrient intake up to day 8 in the pediatric intensive care unit (PICU), accelerated recovery compared to initiating supplemental parenteral nutrition early (early-PN). Whether NTI is harmful or beneficial in pediatric critical illness and how it is affected by a macronutrient deficit remains unclear. This study investigated the prognostic value of NTI, the impact of late-PN on NTI, and whether such impact explains or counteracts the outcome benefit of late-PN in critically ill children.
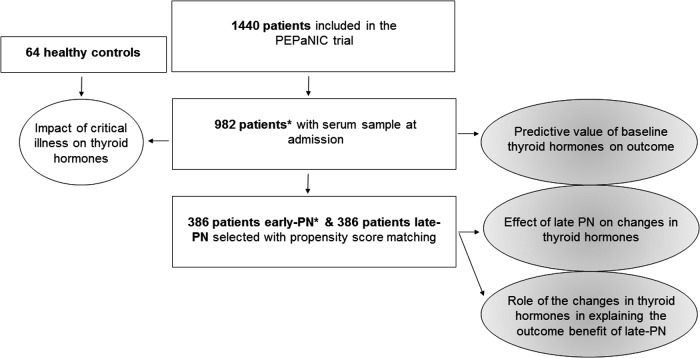
Methods: This preplanned secondary analysis of the Early versus Late Parenteral Nutrition in the Pediatric Intensive Care Unit randomized controlled trial quantified serum TSH, total thyroxine (T4), T3, and rT3 concentrations in 982 patients upon PICU admission versus 64 matched healthy children and in 772 propensity score-matched early-PN and late-PN patients upon admission and at day 3 or last PICU day for shorter PICU stay. Associations between thyroid hormone concentrations upon admission and outcome, as well as impact of late-PN on NTI in relation with outcome, were assessed with univariable analyses and multivariable logistic regression, linear regression, or Cox proportional hazard analysis, adjusted for baseline risk factors.
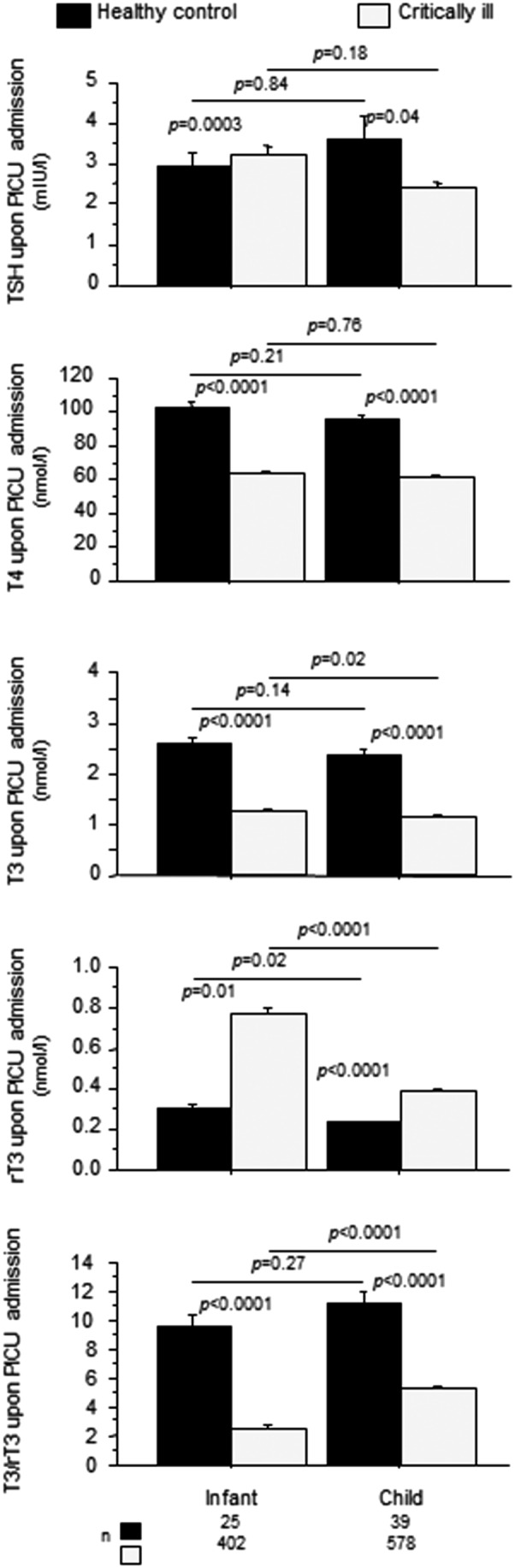
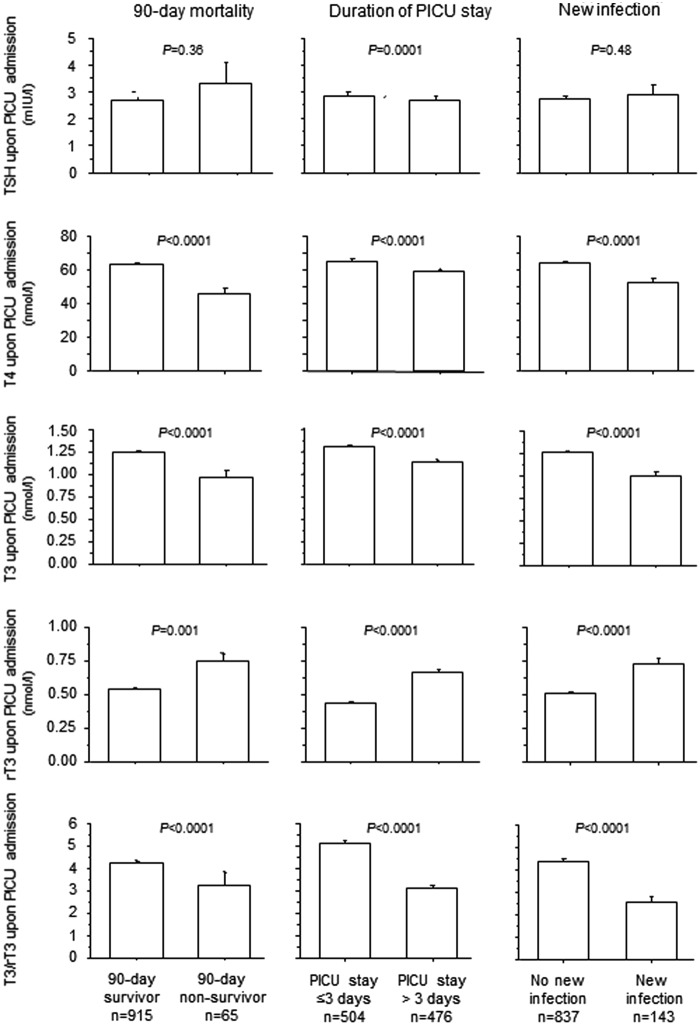
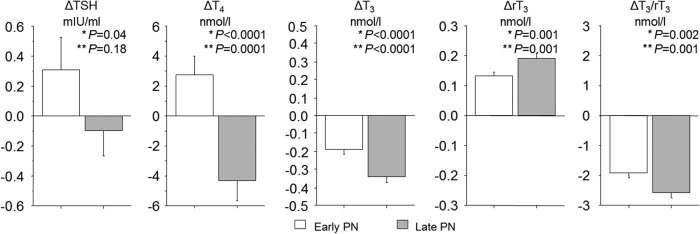
Results: Upon PICU admission, critically ill children revealed lower TSH, T4, T3, and T3/rT3 and higher rT3 than healthy children (p < 0.0001). A more pronounced NTI upon admission, with low T4, T3, and T3/rT3 and high rT3 was associated with higher mortality and morbidity. Late-PN further reduced T4, T3, and T3/rT3 and increased rT3 (p ≤ 0.001). Statistically, the further lowering of T4 by late-PN reduced the outcome benefit (p < 0.0001), whereas the further lowering of T3/rT3 explained part of the outcome benefit of late-PN (p ≤ 0.004). This effect was greater for infants than for older children.
Conclusion: In critically ill children, the peripheral inactivation of thyroid hormone, characterized by a decrease in T3/rT3, which is further accentuated by low/no macronutrient intake, appears beneficial. In contrast, the central component of NTI attributable to suppressed TSH, evidenced by the decrease in T4, seems to be a harmful response to critical illness. Whether treating the central component with TSH releasing hormone infusion in the PICU is beneficial requires further investigation.
Keywords: critical illness; non-thyroidal illness syndrome; nutrition; pediatrics; prognostic value.
Figures
Similar articles
-
Impact of early nutrient restriction during critical illness on the nonthyroidal illness syndrome and its relation with outcome: a randomized, controlled clinical study.J Clin Endocrinol Metab. 2013 Mar;98(3):1006-13. doi: 10.1210/jc.2012-2809. Epub 2013 Jan 24. J Clin Endocrinol Metab. 2013. PMID: 23348400 Clinical Trial.
-
Non-thyroidal illness in the ICU: a syndrome with different faces.Thyroid. 2014 Oct;24(10):1456-65. doi: 10.1089/thy.2014.0201. Epub 2014 Jun 19. Thyroid. 2014. PMID: 24845024 Free PMC article. Review.
-
Outcomes of Delaying Parenteral Nutrition for 1 Week vs Initiation Within 24 Hours Among Undernourished Children in Pediatric Intensive Care: A Subanalysis of the PEPaNIC Randomized Clinical Trial.JAMA Netw Open. 2018 Sep 7;1(5):e182668. doi: 10.1001/jamanetworkopen.2018.2668. JAMA Netw Open. 2018. PMID: 30646158 Free PMC article. Clinical Trial.
-
Leukocyte telomere length in paediatric critical illness: effect of early parenteral nutrition.Crit Care. 2018 Feb 21;22(1):38. doi: 10.1186/s13054-018-1972-6. Crit Care. 2018. PMID: 29463275 Free PMC article.
-
Nonthyroidal illness in critically ill children.Curr Opin Endocrinol Diabetes Obes. 2019 Oct;26(5):241-249. doi: 10.1097/MED.0000000000000494. Curr Opin Endocrinol Diabetes Obes. 2019. PMID: 31343421 Review.
Cited by
-
To study thyroid hormone levels (FT3, FT4, and TSH levels) in critically ill children and their correlation with disease severity and clinical outcome in Rajendra Institute of Medical Sciences, Ranchi, Jharkhand.J Family Med Prim Care. 2022 Oct;11(10):6001-6005. doi: 10.4103/jfmpc.jfmpc_90_22. Epub 2022 Oct 31. J Family Med Prim Care. 2022. PMID: 36618236 Free PMC article.
-
Thyroid Function and Anti-thyroid Antibodies in Pediatric Anti-NMDAR Encephalitis.Front Neurol. 2021 Sep 9;12:707046. doi: 10.3389/fneur.2021.707046. eCollection 2021. Front Neurol. 2021. PMID: 34566852 Free PMC article.
-
Nonthyroidal Illness Syndrome Across the Ages.J Endocr Soc. 2019 Oct 16;3(12):2313-2325. doi: 10.1210/js.2019-00325. eCollection 2019 Dec 1. J Endocr Soc. 2019. PMID: 31745528 Free PMC article. Review.
-
Analysis of the Incidence of Euthyroid Sick Syndrome in Comprehensive Intensive Care Units and Related Risk Factors.Front Endocrinol (Lausanne). 2021 Jun 9;12:656641. doi: 10.3389/fendo.2021.656641. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34177801 Free PMC article.
-
Thyroid Hormones Interaction With Immune Response, Inflammation and Non-thyroidal Illness Syndrome.Front Cell Dev Biol. 2021 Jan 21;8:614030. doi: 10.3389/fcell.2020.614030. eCollection 2020. Front Cell Dev Biol. 2021. PMID: 33553149 Free PMC article. Review.
References
-
- Faber J, Kirkegaard C, Rasmussen B, Westh H, Busch-Sorensen M, Jensen IW. 1987. Pituitary–thyroid axis in critical illness. J Clin Endocrinol Metab 65:315–320 - PubMed
-
- Murzi B, Iervasi G, Masini S, Moschetti R, Vanini V, Zucchelli G, Biagini A. 1995. Thyroid hormones homeostasis in pediatric patients during and after cardiopulmonary bypass. Ann Thorac Surg 59:481–485 - PubMed
-
- Van den Berghe G, de Zegher F, Lauwers P. 1994. Dopamine suppresses pituitary function in infants and children. Crit Care Med 22:1747–1753 - PubMed
-
- Uzel N, Neyzi O. 1986. Thyroid function in critically ill infants with infections. Pediatr Infect Dis 5:516–519 - PubMed
-
- Allen DB, Dietrich KA, Zimmerman JJ. 1989. Thyroid hormone metabolism and level of illness severity in pediatric cardiac surgery patients. J Pediatr 114:59–62 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
