

The effect of SENATOR (Software ENgine for the Assessment and optimisation of drug and non-drug Therapy in Older peRsons) on incident adverse drug reactions (ADRs) in an older hospital cohort - Trial Protocol
- PMID: 30760204
- PMCID: PMC6375169
- DOI: 10.1186/s12877-019-1047-9
The effect of SENATOR (Software ENgine for the Assessment and optimisation of drug and non-drug Therapy in Older peRsons) on incident adverse drug reactions (ADRs) in an older hospital cohort - Trial Protocol
Abstract
Background: The aim of this trial is to evaluate the effect of SENATOR software on incident, adverse drug reactions (ADRs) in older, multimorbid, hospitalized patients. The SENATOR software produces a report designed to optimize older patients' current prescriptions by applying the published STOPP and START criteria, highlighting drug-drug and drug-disease interactions and providing non-pharmacological recommendations aimed at reducing the risk of incident delirium.
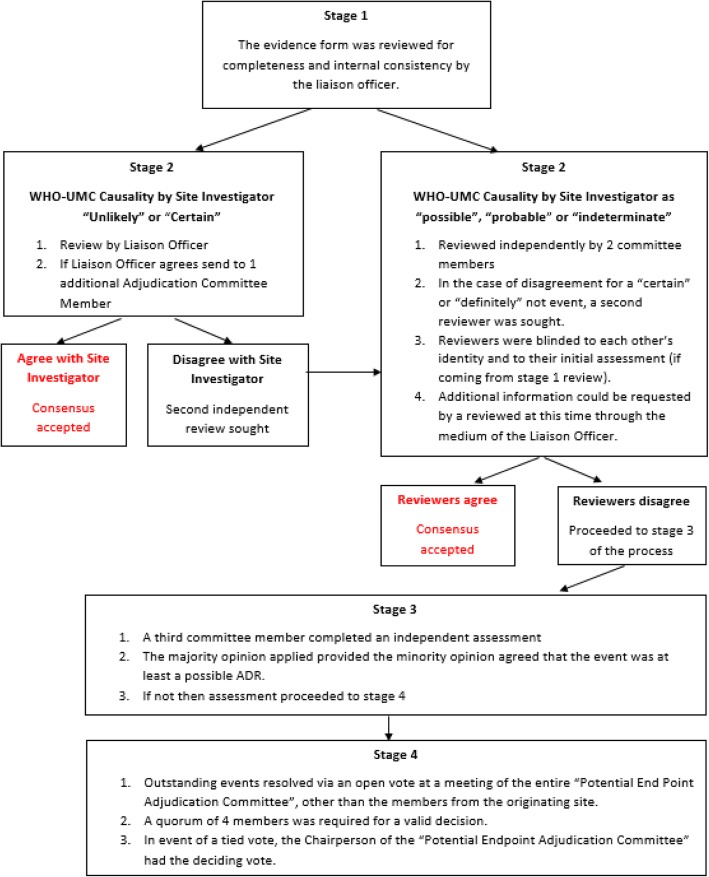
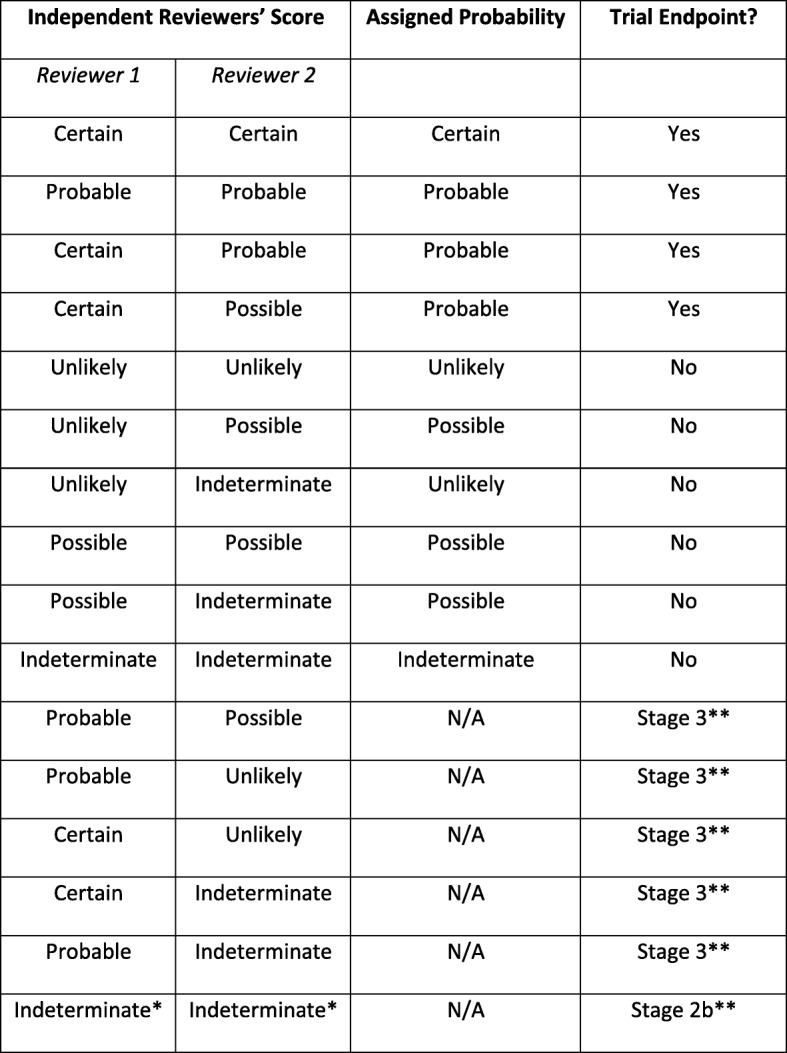
Methods: We will conduct a multinational, pragmatic, parallel arm Prospective Randomized Open-label, Blinded Endpoint (PROBE) controlled trial. Patients with acute illnesses are screened for recruitment within 48 h of arrival to hospital and enrolled if they meet the relevant entry criteria. Participants' medical history, current prescriptions, select laboratory tests, electrocardiogram, cognitive status and functional status are collected and entered into a dedicated trial database. Patients are individually randomized with equal allocation ratio. Randomization is stratified by site and medical versus surgical admission, and uses random block sizes. Patients randomized to either arm receive standard routine pharmaceutical clinical care as it exists in each site. Additionally, in the intervention arm an individualized SENATOR-generated medication advice report based on the participant's clinical and medication data is placed in their medical record and a senior medical staff member is requested to review it and adopt any of its recommendations that they judge appropriate. The trial's primary outcome is the proportion of patients experiencing at least one adjudicated probable or certain, non-trivial ADR, during the index hospitalization, assessed at 14 days post-randomization or at index hospital discharge if it occurs earlier. Potential ADRs are identified retrospectively by the site researchers who complete a Potential Endpoint Form (one per type of event) that is adjudicated by a blinded, expert committee. All occurrences of 12 pre-specified events, which represent the majority of ADRs, are reported to the committee along with other suspected ADRs. Participants are followed up 12 (+/- 4) weeks post-index hospital discharge to assess medication quality and healthcare utilization. This is the first clinical trial to examine the effectiveness of a software intervention on incident ADRs and associated healthcare costs during hospitalization in older people with multi-morbidity and polypharmacy.
Trial registration number: Clinicaltrials.gov NCT02097654 , 27 March 2014.
Keywords: Adverse drug reactions; Computer software; Hospitalization; Intervention study; Medication alert systems; Multimorbidity; Older adults; Polypharmacy; Randomized controlled trial.
Conflict of interest statement
Ethics approval and consent to participate
The patient information leaflet and informed consent documents were developed in the Trial Coordinating Centre, based in the Clinical Research Facility, Cork and approved by the Clinical Research Ethics Committee of the Cork Teaching Hospitals, (ref ECM 3 O’Mahony SENATOR 08122015). These were then translated by Site Investigators, modified as needed to meet local requirements and submitted, reviewed and approved by the local ethics committees as follows:
Research Ethics Committee, Aberdeen, Scotland; R
Comitato Ethics Azienda Ospedaliers-Universitaria Ospedali Riuniti, Italy. Ref
Universitair Ziekenhuis, Gent Belgium. Ref:
Comité Etico de Investigacion Clinica de Hospital Ramon y Cajal, Madrid, Spain. Ref: 382/12.
Research Ethics Committee Reykjavík, Iceland R
Written informed consent will be obtained by trial study staff from all participants or authorized surrogates as per local legislation and ethics committee approval. Potential participants were identified, reviewed with their clinical team and provided with study documentation. Any questions were answered and informed written consent was obtained.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
