

Patient satisfaction of radiofrequency ablation for symptomatic benign solid thyroid nodules: our experience for 2-year follow up
- PMID: 30760229
- PMCID: PMC6375217
- DOI: 10.1186/s12885-019-5338-5
Patient satisfaction of radiofrequency ablation for symptomatic benign solid thyroid nodules: our experience for 2-year follow up
Abstract
Background: The patient satisfaction of symptoms improvement and disease factors that may affect long-term treatment efficacy of radiofrequency ablation (RFA) for non-functioning solid benign thyroid nodules (TNs) over a 2-year follow up study was investigated.
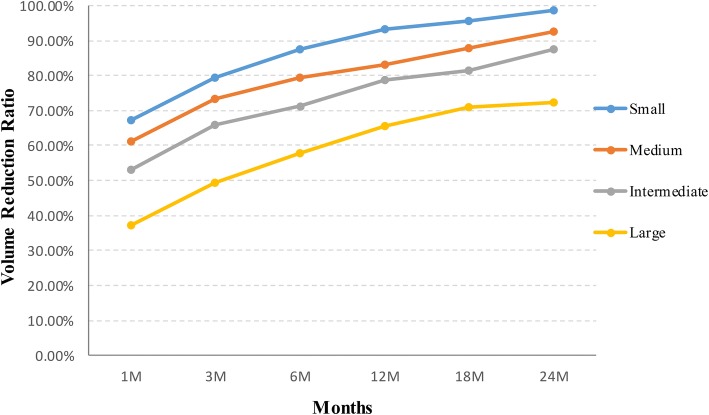
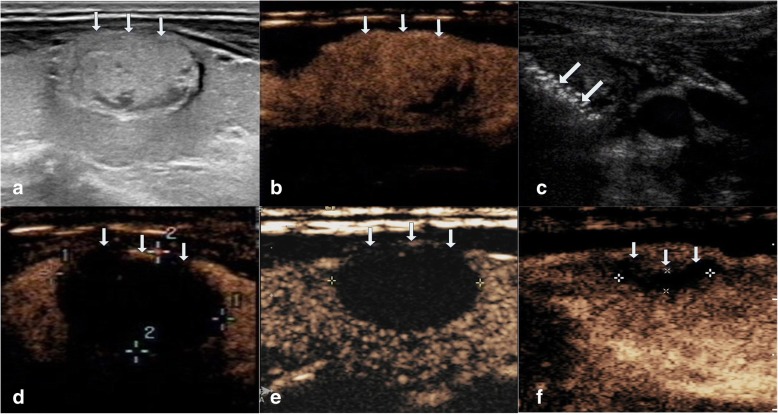
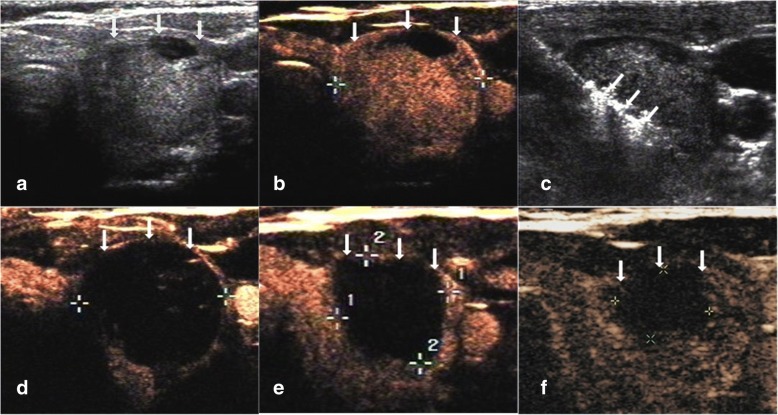
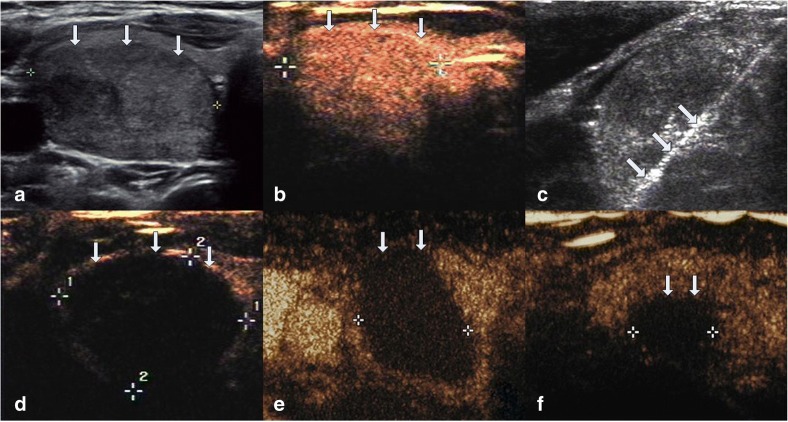
Methods: This retrospective study evaluated 194 non-functioning solid benign TNs of 103 patients. The TNs were categorized as small (≤5 ml), medium (5.1 to 13 ml), intermediate (13.1 to 30 ml) and large (over 30 ml) according to the initial volume of TNs before ablation. Clinical evaluation and contrast-enhanced ultrasound (CEUS) were carried out before ablation and the follow up at 1, 3, 6 months and every 6 months after ablation. All patients were asked to assess the cosmetic score (1-4 scores) and symptom score (0-10 scores) before ablation and every follow up after ablation.
Results: All patients underwent RFA without any major complications. The mean treatment sessions were 1.5 ± 0.6. 98 nodules required a single session (98/194, 50.5%), 87 required two sessions (87/194, 44.9%), 9 required three sessions (9/194, 4.6%). The average follow up months were 16.3 ± 5.6 (range, 6-24 months) and no nodule regrew in our study. After RFA treatment, the TNs volume significantly decreased (P < 0.001). The small group of nodules shrunk larger compared to the medium, intermediate and large groups (P < 0.001). Cosmetic signs and pressure symptoms were significantly improved, particularly in the intermediate and large groups (P < 0.05).
Conclusions: RFA is effective for treating non-functioning solid benign TNs and controlling clinical symptoms with a low complication rate during 2 years follow up. The reduction rate was related to the initial volume of nodules. Patients were satisfied with cosmetic signs and pressure symptoms improvement, particularly in the intermediate and large groups. However, multiple RFA treatments should be used in larger nodules to achieve the desired clinical outcomes.
Keywords: Radiofrequency ablation (RFA); Thyroid nodules; Ultrasound.
Conflict of interest statement
Ethics approval and consent to participate
The protocol was approved by the Institutional Review Board of the Beijing Tian Tan Hospital Ethics Committee and the Chinese PLA General Hospital Ethics Committee. All subjects provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
