

Improved long-term survival with home hemodialysis compared with institutional hemodialysis and peritoneal dialysis: a matched cohort study
- PMID: 30760251
- PMCID: PMC6375181
- DOI: 10.1186/s12882-019-1245-x
Improved long-term survival with home hemodialysis compared with institutional hemodialysis and peritoneal dialysis: a matched cohort study
Abstract
Background: The survival rate for dialysis patients is poor. Previous studies have shown improved survival with home hemodialysis (HHD), but this could be due to patient selection, since HHD patients tend to be younger and healthier. The aim of the present study is to analyse the long-term effects of HHD on patient survival and on subsequent renal transplantation, compared with institutional hemodialysis (IHD) and peritoneal dialysis (PD), taking age and comorbidity into account.
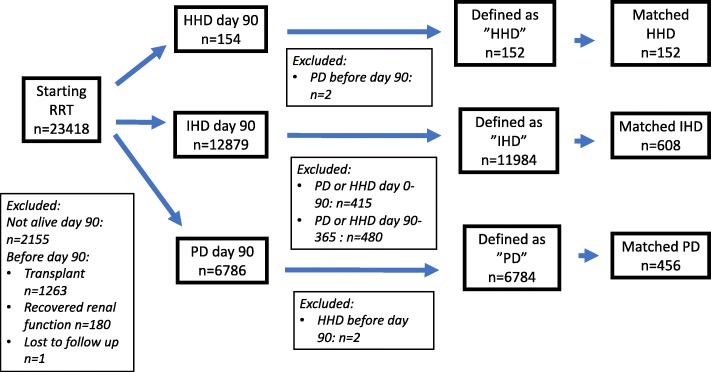
Methods: Patients starting HHD as initial renal replacement therapy (RRT) were matched with patients on IHD or PD, according to gender, age, Charlson Comorbidity Index and start date of RRT, using the Swedish Renal Registry from 1991 to 2012. Survival analyses were performed as intention-to-treat (disregarding changes in RRT) and per-protocol (as on initial RRT).
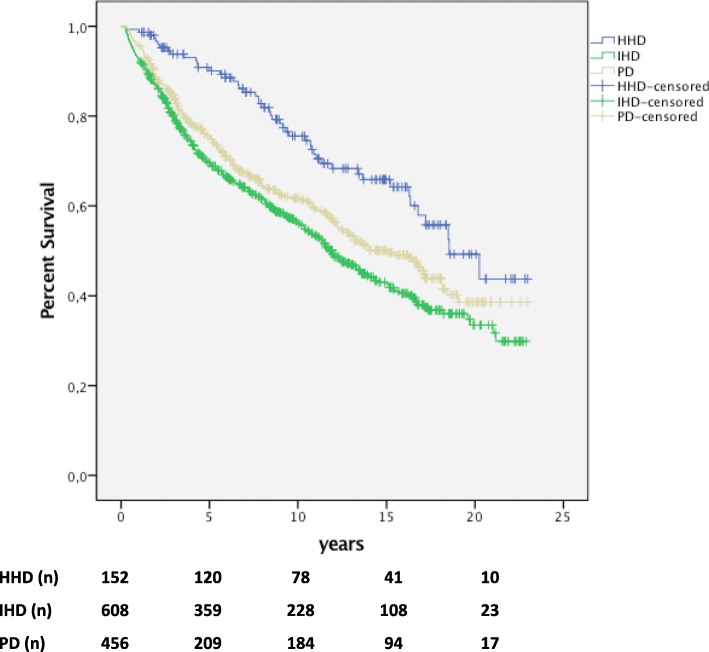
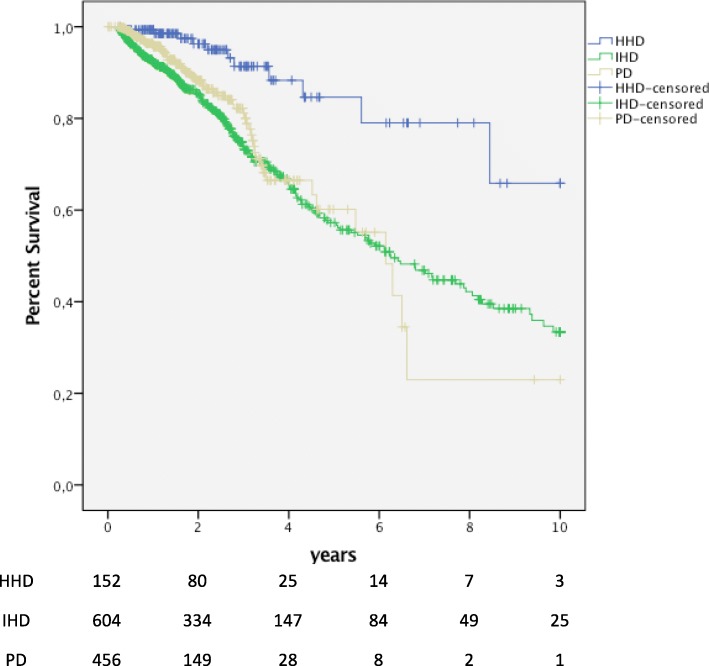
Results: A total of 152 patients with HHD as initial RRT were matched with 608 IHD and 456 PD patients, respectively. Median survival was longer for HHD in intention-to-treat analyses: 18.5 years compared with 11.9 for IHD (p < 0.001) and 15.0 for PD (p = 0.002). The difference remained significant in per-protocol analyses omitting the contribution of subsequent transplantation. Patients on HHD were more likely to receive a renal transplant compared with IHD and PD, although treatment modality did not affect subsequent graft survival (p > 0.05).
Conclusion: HHD as initial RRT showed improved long-term patient survival compared with IHD and PD. This survival advantage persisted after matching and adjusting for a higher transplantation rate. Dialysis modality had no impact on subsequent graft survival.
Keywords: Home hemodialysis; Institutional hemodialysis; Peritoneal dialysis; Renal graft survival; Survival.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Regional Ethical Review Board in Lund (2014/933). In this study we only used registry data. According to Swedish law Quality Registries can be used for research. Patients are informed and have a right to decline to be registered, but no additional consent is required for specific projects.
Consent for publication
Not applicable.
Competing interests
he authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- USRDS Annual report 2016. https://www.usrds.org.
-
- ERA-EDTA Annual report 2015. https://www.era-edta-reg.org.
-
- Swedish Renal Registry Annual Report 2016. https://www.medscinet.net/snr.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
