

Pracinostat plus azacitidine in older patients with newly diagnosed acute myeloid leukemia: results of a phase 2 study
- PMID: 30760466
- PMCID: PMC6391673
- DOI: 10.1182/bloodadvances.2018027409
Pracinostat plus azacitidine in older patients with newly diagnosed acute myeloid leukemia: results of a phase 2 study
Abstract
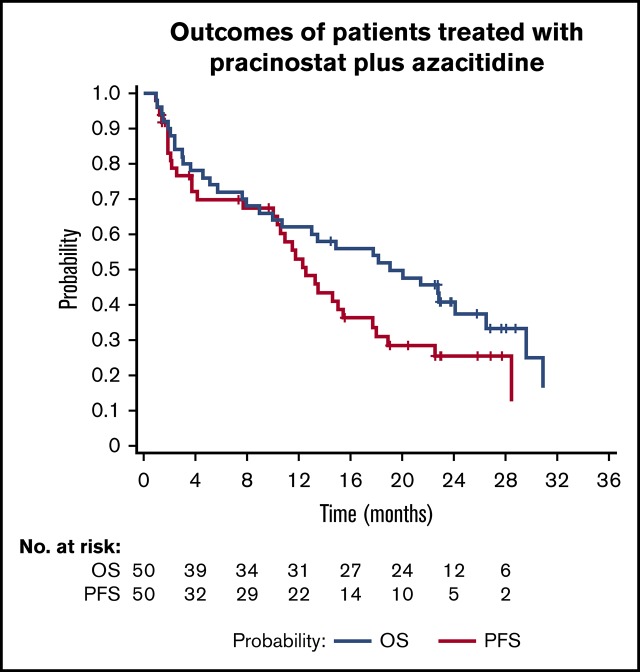
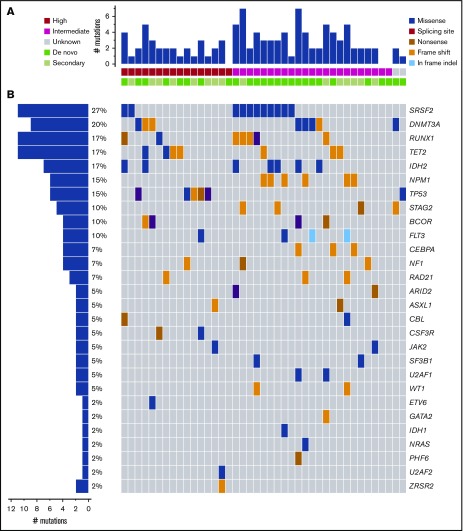
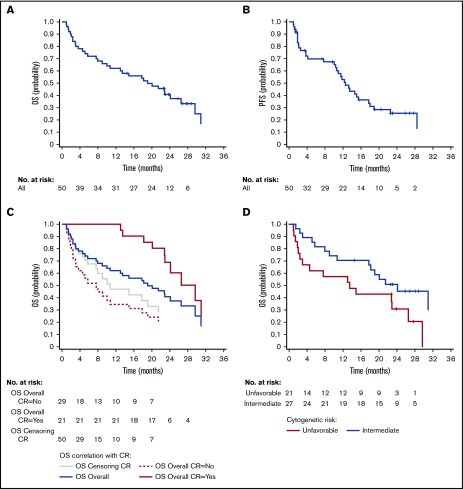
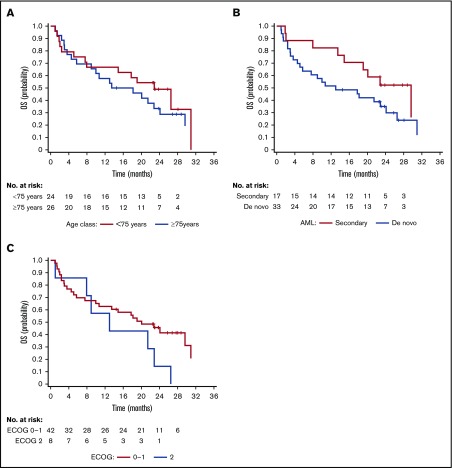
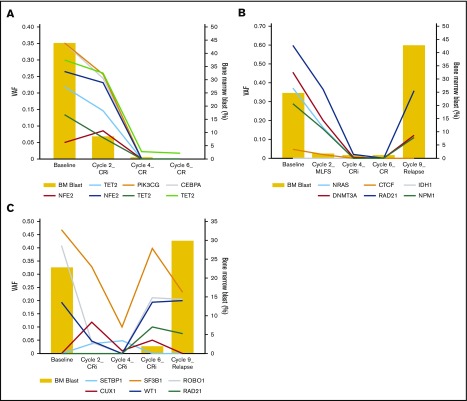
Pracinostat, a potent oral pan-histone deacetylase inhibitor with modest single-agent activity in acute myeloid leukemia (AML), has shown synergistic antitumor activity when combined with azacitidine. This single-group, multicenter phase 2 study assessed the safety and efficacy of pracinostat combined with azacitidine in patients who were at least 65 years old with newly diagnosed AML and who were ineligible for standard induction chemotherapy. Patients received pracinostat 60 mg/d, 3 d/wk, for 3 consecutive weeks, plus azacitidine 75 mg/m2 daily for 7 days in a 28-day cycle. Primary endpoints were complete remission (CR), CR with incomplete count recovery (CRi), and morphologic leukemia-free state (MLFS) rates of the combination. Secondary endpoints included safety, progression-free survival (PFS), and overall survival (OS) of the regimen. Fifty patients (33 de novo, 12 secondary, and 5 therapy-related AML) were enrolled. Twenty-six patients (52%) achieved the primary endpoint of CR (42%), CRi (4%), and MLFS (6%). Median OS and PFS were 19.1 months (95% confidence interval [CI], 10-26.5 months) and 12.6 months (95% CI, 10-17.7 months), respectively, with a 1-year OS rate of 62%. Forty-three patients (86%) experienced at least 1 grade 3 or worse treatment-emergent adverse event with the combination, with infections (52%), thrombocytopenia (46%), and febrile neutropenia (44%) reported as the most common toxicities. The 30- and 60-day all-cause mortality rates were 2% and 10%, respectively. DNA sequencing revealed somatic mutations at baseline, and clearance rates correlated with response to treatment. Pracinostat plus azacitidine is a well-tolerated and active regimen in the frontline treatment of older patients with AML unfit for intensive therapy. A larger controlled trial is ongoing. This trial was registered at www.clinicaltrials.gov as #NCT01912274.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: K.T. has received honoraria from Kyowa Hakko Kirin, Celgene, and Pharmacyclics; has served as a consultant or advisor for SymBio Pharmaceuticals; has received research funding from Onconova Therapeutics and MEI Pharma; has received travel, accommodations, and expenses from SymBio Pharmaceuticals and Helsinn Therapeutics. S.K.K. has received honoraria and has served as a consultant or advisor for Alexion and Daiichi and has served on the speakers’ bureau for Alexion. O.O. has received honoraria from AbbVie Pharmaceuticals; has served as a consultant or advisor for Pfizer, Celgene, CTI/Baxalta, Dava Oncology, Incyte Pharmaceuticals, and Jazz Pharmaceuticals; and has received research funding from AbbVie, Oncotherapy Science, CTI BioPharma, Agios Pharmaceuticals, Celgene Corporation, NS Pharma, Janssen Research and Development, Astex Pharmaceuticals, and Gilead Sciences. P.P. has received honoraria from Dava Oncology and France Foundation, has served as a consultant or advisor for Celgene, and has served on the speakers’ bureau for Celgene. R.S. has received research funding from Ono Pharmaceuticals. E.T. has received honoraria from Astellas; has served as a consultant or advisor for Astellas, Agios, ImmunoGen, and Tolero; and has received research funding from Astellas and Janssen. K.K. has received honoraria from Incyte, Bristol-Myers Squibb, Celgene, Takeda, and Genentech/Roche; and has served on the speakers’ bureau for Incyte, Bristol-Myers Squibb, Celgene, Novartis, and Takeda. A.Y. has stock or other ownership in Dynavax, Cara, and Ardelyx; has received honoraria from Incyte and Seattle Genetics; and has served on the speakers’ bureau for Incyte, Seattle Genetics, and Novartis. R. Ghalie is an employee of MEI Pharma Inc. R. Giorgino is employed by and holds a leadership role in Helsinn Healthcare. E.A. has received research funding from Takeda and honoraria from Ariad, Jazz, AbbVie, and Pfizer; has served as a consultant for BMS, Novartis, CIT Biopharma, and Incyte; and has served as a grant reviewer for Pfizer. The remaining authors declare no competing financial interests.
Figures
References
-
- O’Donnell MR, Tallman MS, Abboud CN, et al. Acute myeloid leukemia, version 3.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15(7):926-957. - PubMed
-
- Anderson JE, Kopecky KJ, Willman CL, et al. Outcome after induction chemotherapy for older patients with acute myeloid leukemia is not improved with mitoxantrone and etoposide compared to cytarabine and daunorubicin: a Southwest Oncology Group study. Blood. 2002;100(12):3869-3876. - PubMed
-
- Dombret H, Raffoux E, Gardin C. Acute myeloid leukemia in the elderly. Semin Oncol. 2008;35(4):430-438. - PubMed
-
- Gardin C, Turlure P, Fagot T, et al. Postremission treatment of elderly patients with acute myeloid leukemia in first complete remission after intensive induction chemotherapy: results of the multicenter randomized Acute Leukemia French Association (ALFA) 9803 trial. Blood. 2007;109(12):5129-5135. - PubMed
