

Surgical Intervention for Osteoporotic Vertebral Burst Fractures in Middle-low Lumbar Spine with Special Reference to Postoperative Complications Affecting Surgical Outcomes
- PMID: 30760656
- PMCID: PMC6434421
- DOI: 10.2176/nmc.oa.2018-0232
Surgical Intervention for Osteoporotic Vertebral Burst Fractures in Middle-low Lumbar Spine with Special Reference to Postoperative Complications Affecting Surgical Outcomes
Abstract
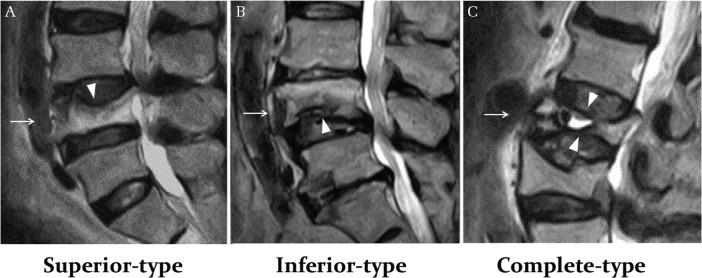
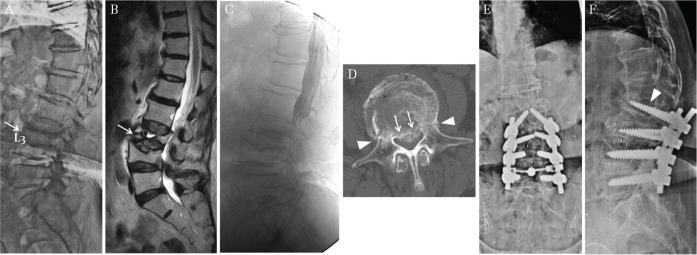
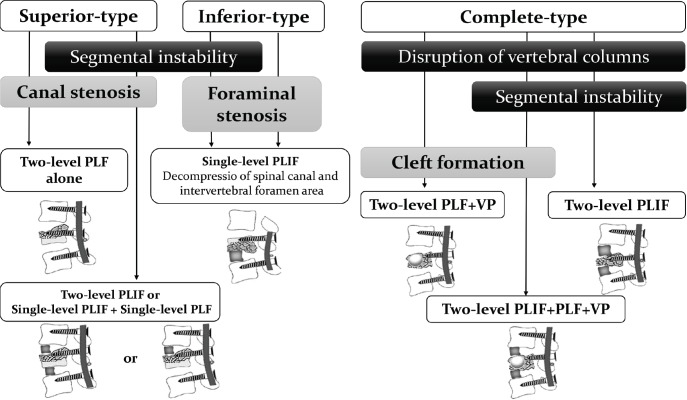
The purpose of this study was to investigate the clinical and radiological features of osteoporotic burst fractures affecting levels below the second lumbar (middle-low lumbar) vertebrae, and to clarify the appropriate surgical procedure to avoid postoperative complications. Thirty-eight consecutive patients (nine male, 29 female; mean age: 74.8 years; range: 60-86 years) with burst fractures affecting the middle-low lumbar vertebrae who underwent posterior-instrumented fusion were included. Using the Magerl classification system, these fractures were classified into three types: 16 patients with superior incomplete burst fracture (superior-type), 11 patients with inferior incomplete burst fracture (inferior-type) and 11 patients with complete burst fracture (complete-type). The clinical features were investigated for each type, and postoperative complications such as postoperative vertebral collapse (PVC) and instrumentation failure were assessed after a mean follow-up period of 3.1 years (range: 1-8.1 years). All patients suffered from severe leg pain by radiculopathy, except one with superior-type fracture who exhibited cauda equina syndrome. Nineteen of 27 patients with superior- or inferior-type fracture were found to have spondylolisthesis due to segmental instability. Although postoperative neurological status improved significantly, lumbar lordosis and segmental lordosis at the fused level deteriorated from the postoperative period to the final follow-up due to postoperative complications caused mainly by PVC (29%) and instrument failure (37%). Posterior-instrumented fusion led to a good clinical outcome; however, a higher incidence of postoperative complications due to bone fragility was inevitable. Therefore, short-segment instrument and fusion with some augumentation techniqus, together with strong osteoporotic medications may be required to avoid such complications.
Keywords: middle-low lumbar spine; osteoporotic vertebral burst fracture; posterior decompression and fusion.
Conflict of interest statement
All authors have no conflict of interest.
Figures
References
-
- Sasaki M, Aoki M, Nishioka K, Yoshimine T: Radiculopathy caused by osteoporotic vertebral fractures in the lumbar spine. Neurol Med Chir (Tokyo) 51: 484–489, 2011 - PubMed
-
- Nakajima H, Uchida K, Honjoh K, Sakamoto T, Kitade M, Baba H: Surgical treatment of low lumbar osteoporotic vertebral collapse: a single-institution experience. J Neurosurg Spine 24: 39–47, 2016 - PubMed
-
- Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S: A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 3: 184–201, 1994 - PubMed