

Predicting Alzheimer's disease progression using multi-modal deep learning approach
- PMID: 30760848
- PMCID: PMC6374429
- DOI: 10.1038/s41598-018-37769-z
Predicting Alzheimer's disease progression using multi-modal deep learning approach
Erratum in
-
Author Correction: Predicting Alzheimer's disease progression using multi-modal deep learning approach.Sci Rep. 2023 Aug 1;13(1):12466. doi: 10.1038/s41598-023-39138-x. Sci Rep. 2023. PMID: 37528098 Free PMC article. No abstract available.
Abstract
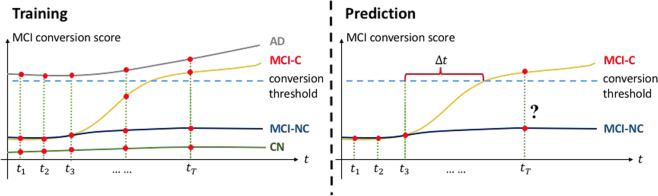
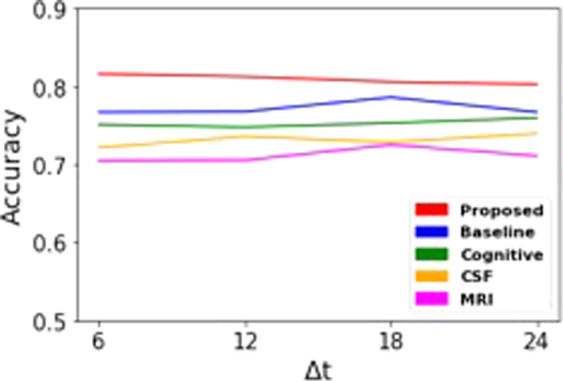
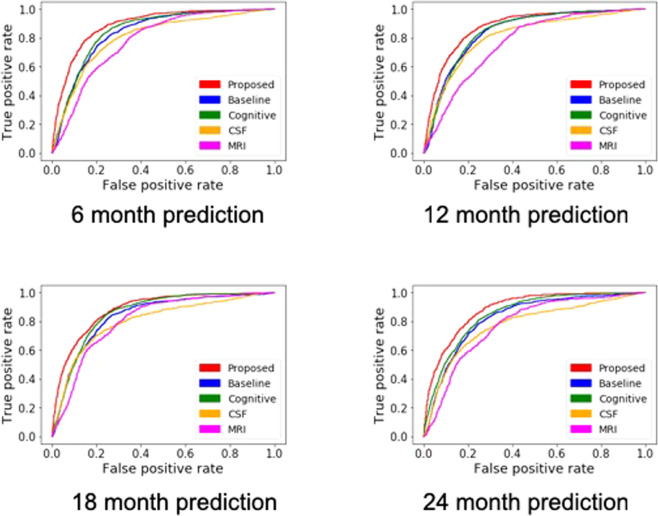
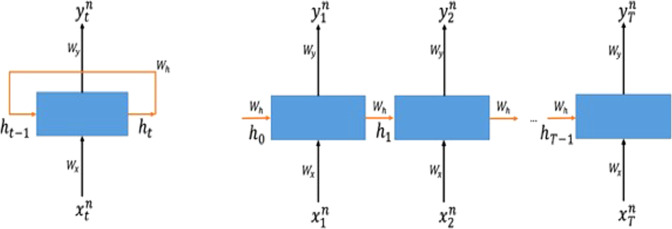
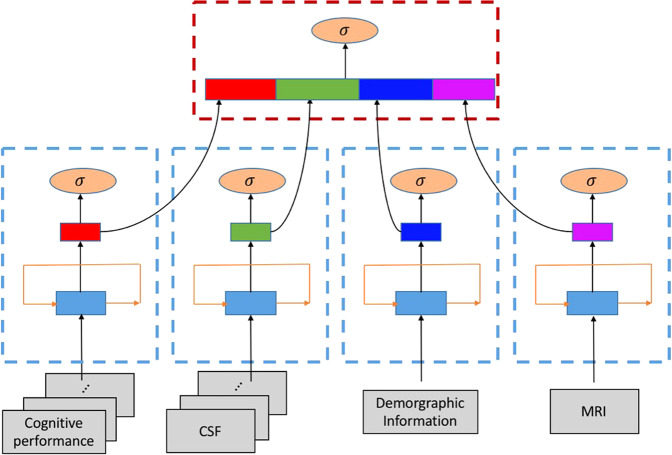
Alzheimer's disease (AD) is a progressive neurodegenerative condition marked by a decline in cognitive functions with no validated disease modifying treatment. It is critical for timely treatment to detect AD in its earlier stage before clinical manifestation. Mild cognitive impairment (MCI) is an intermediate stage between cognitively normal older adults and AD. To predict conversion from MCI to probable AD, we applied a deep learning approach, multimodal recurrent neural network. We developed an integrative framework that combines not only cross-sectional neuroimaging biomarkers at baseline but also longitudinal cerebrospinal fluid (CSF) and cognitive performance biomarkers obtained from the Alzheimer's Disease Neuroimaging Initiative cohort (ADNI). The proposed framework integrated longitudinal multi-domain data. Our results showed that 1) our prediction model for MCI conversion to AD yielded up to 75% accuracy (area under the curve (AUC) = 0.83) when using only single modality of data separately; and 2) our prediction model achieved the best performance with 81% accuracy (AUC = 0.86) when incorporating longitudinal multi-domain data. A multi-modal deep learning approach has potential to identify persons at risk of developing AD who might benefit most from a clinical trial or as a stratification approach within clinical trials.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Albert MS, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:270–279. doi: 10.1016/j.jalz.2011.03.008. - DOI - PMC - PubMed
-
- Sperling RA, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:280–292. doi: 10.1016/j.jalz.2011.03.003. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
