

Comparison of Two Respiratory Support Strategies for Stabilization of Very Preterm Infants at Birth: A Matched-Pairs Analysis
- PMID: 30761276
- PMCID: PMC6362425
- DOI: 10.3389/fped.2019.00003
Comparison of Two Respiratory Support Strategies for Stabilization of Very Preterm Infants at Birth: A Matched-Pairs Analysis
Abstract
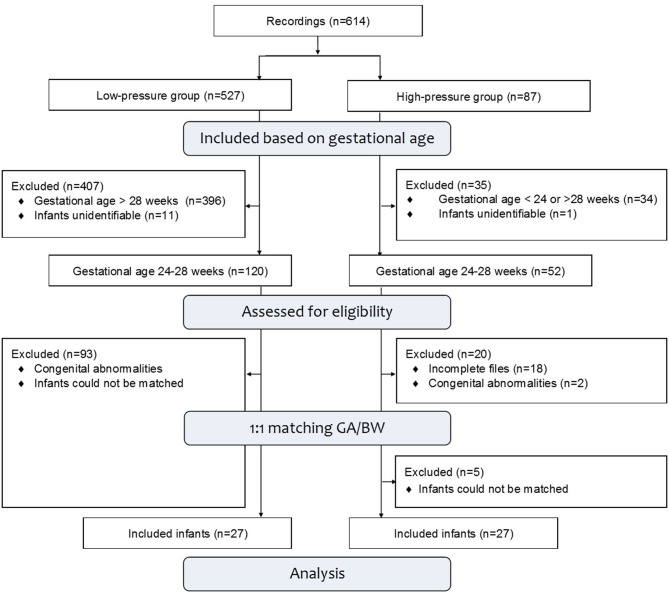
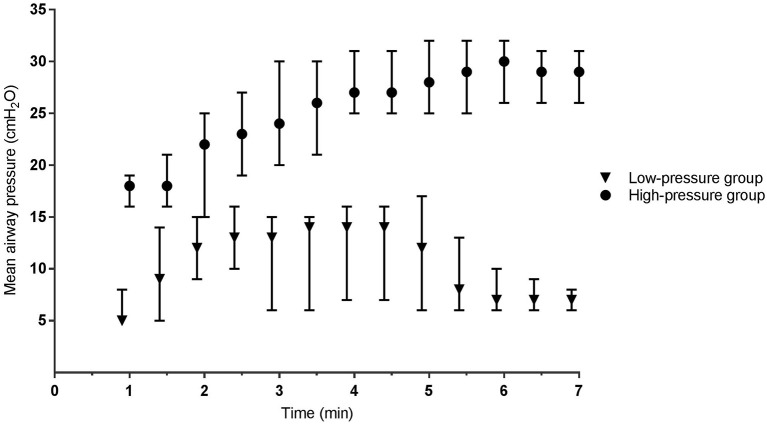
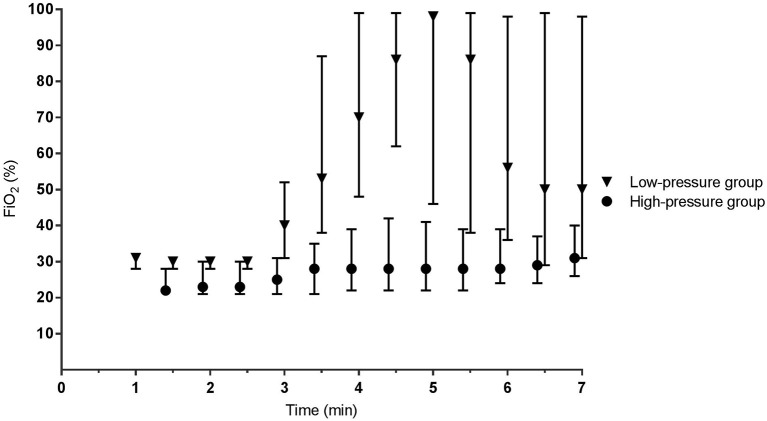
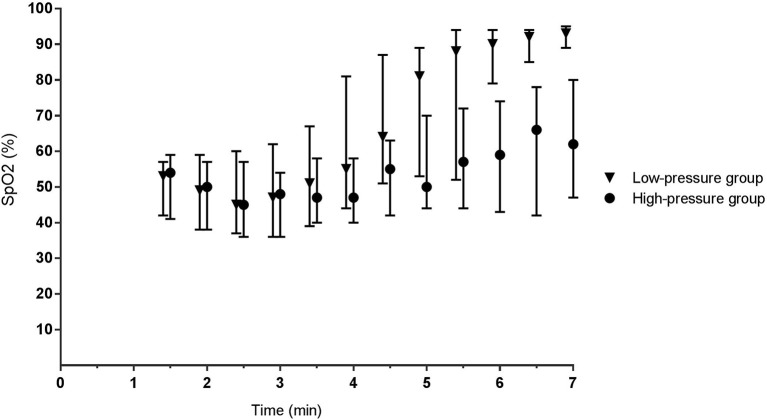
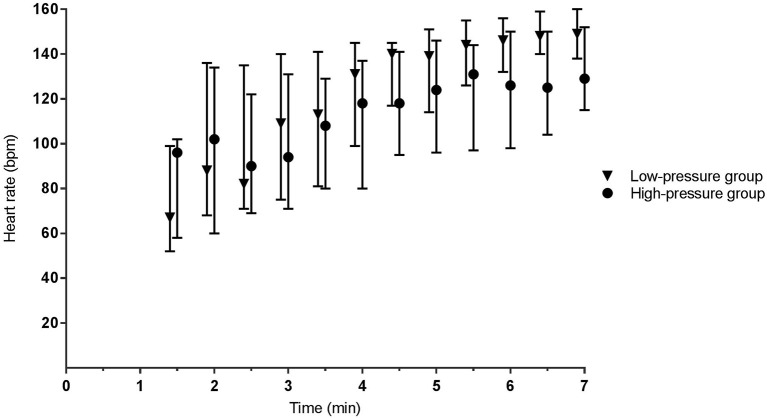
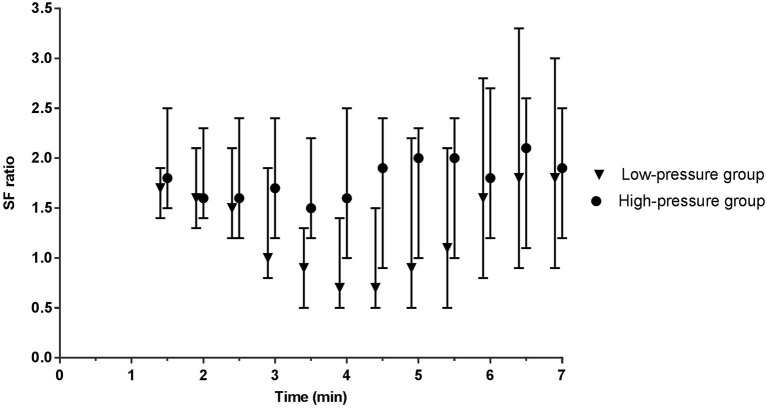
Objective: Respiratory support for stabilizing very preterm infants at birth varies between centers. We retrospectively compared two strategies that involved either increasing continuous positive airway pressures (CPAP), or increasing oxygen supplementation. Methods: Matched-pairs of infants (<28 weeks of gestation) were born either at the Leiden University Medical Center [low-pressure: CPAP 5-8 cmH2O and/or positive pressure ventilation (PPV) and fraction of inspired oxygen (FiO2) 0.3-1.0; n = 27], or at the University Hospital of Cologne (high-pressure: CPAP 12-35 cmH2O, no PPV and FiO2 0.3-0.4; n = 27). Respiratory support was initiated non-invasively via facemask at both units. Infants (n = 54) were matched between centers for gestational age and birth weight, to compare physiological and short-term clinical outcomes. Results: In the low-pressure group, 20/27 (74%) infants received 1-2 sustained inflations (20, 25 cm H2O) and 22/27 (81%) received PPV (1:19-3:01 min) using pressures of 25-27 cm H2O. Within 3 min of birth [median (IQR)], mean airway pressures [12 (6-15) vs. 19 (16-23) cmH2O, p < 0.001] and FiO2 [0.30 (0.28-0.31) vs. 0.22 (0.21-0.30), p < 0.001] were different in low- vs. high-pressure groups, respectively. SpO2 and heart rates were similar. After 3 min, higher FiO2 levels [0.62 (0.35-0.98) vs. 0.28 (0.22-0.38), p = 0.005] produced higher SpO2 levels [77 (50-92) vs. 53 (42-69)%, p < 0.001] in the low-pressure group, but SpO2/FiO2 and heart rates were similar. While intubation rates during admission were significantly different (70 vs. 30%, p = 0.013), pneumothorax rates (4 vs. 19%, p = 0.125) and the occurrence of spontaneous intestinal perforations (0 vs. 15%, p = 0.125) were similar between groups. Conclusion: Infants (<28 weeks) can be supported non-invasively at birth with either higher or lower pressures and while higher-pressure support may require less oxygen, it does not eliminate the need for oxygen supplementation. Future studies need to examine the effect of high pressures and pressure titration in the delivery room.
Keywords: CPAP; birth; breathing; preterm infants; respiratory support.
Figures
Similar articles
-
Optimising CPAP and oxygen levels to support spontaneous breathing in preterm rabbits.Pediatr Res. 2025 Jan 18. doi: 10.1038/s41390-025-03802-x. Online ahead of print. Pediatr Res. 2025. PMID: 39827256
-
Feasibility and Effect of Physiological-Based CPAP in Preterm Infants at Birth.Front Pediatr. 2021 Dec 3;9:777614. doi: 10.3389/fped.2021.777614. eCollection 2021. Front Pediatr. 2021. PMID: 34926350 Free PMC article.
-
Oxygen saturation after birth in preterm infants treated with continuous positive airway pressure and air: assessment of gender differences and comparison with a published nomogram.Arch Dis Child Fetal Neonatal Ed. 2013 May;98(3):F228-32. doi: 10.1136/archdischild-2012-302369. Epub 2012 Nov 3. Arch Dis Child Fetal Neonatal Ed. 2013. PMID: 23123635
-
Supporting breathing of preterm infants at birth: a narrative review.Arch Dis Child Fetal Neonatal Ed. 2019 Jan;104(1):F102-F107. doi: 10.1136/archdischild-2018-314898. Epub 2018 Jul 26. Arch Dis Child Fetal Neonatal Ed. 2019. PMID: 30049727 Review.
-
Oxygen Supplementation During Preterm Stabilization and the Relevance of the First 5 min After Birth.Front Pediatr. 2020 Jan 31;8:12. doi: 10.3389/fped.2020.00012. eCollection 2020. Front Pediatr. 2020. PMID: 32083039 Free PMC article. Review.
Cited by
-
An Immature Science: Intensive Care for Infants Born at ≤23 Weeks of Gestation.J Pediatr. 2021 Jun;233:16-25.e1. doi: 10.1016/j.jpeds.2021.03.006. Epub 2021 Mar 7. J Pediatr. 2021. PMID: 33691163 Free PMC article. Review. No abstract available.
-
Individualized dynamic PEEP (dynPEEP) vs. positive pressure ventilation in delivery room management: A retrospective cohort study.Front Pediatr. 2023 Jan 11;10:1007632. doi: 10.3389/fped.2022.1007632. eCollection 2022. Front Pediatr. 2023. PMID: 36714644 Free PMC article.
-
Evaluating Clinical Outcomes and Physiological Perspectives in Studies Investigating Respiratory Support for Babies Born at Term With or at Risk of Transient Tachypnea: A Narrative Review.Front Pediatr. 2022 Jun 23;10:878536. doi: 10.3389/fped.2022.878536. eCollection 2022. Front Pediatr. 2022. PMID: 35813383 Free PMC article. Review.
-
Extrauterine Placental Perfusion and Oxygenation in Infants With Very Low Birth Weight: A Randomized Clinical Trial.JAMA Netw Open. 2023 Nov 1;6(11):e2340597. doi: 10.1001/jamanetworkopen.2023.40597. JAMA Netw Open. 2023. PMID: 37921769 Free PMC article. Clinical Trial.
-
Optimising CPAP and oxygen levels to support spontaneous breathing in preterm rabbits.Pediatr Res. 2025 Jan 18. doi: 10.1038/s41390-025-03802-x. Online ahead of print. Pediatr Res. 2025. PMID: 39827256
References
LinkOut - more resources
Full Text Sources