

Intracellular Streptococcal Uptake and Persistence: A Potential Cause of Erysipelas Recurrence
- PMID: 30761303
- PMCID: PMC6361840
- DOI: 10.3389/fmed.2019.00006
Intracellular Streptococcal Uptake and Persistence: A Potential Cause of Erysipelas Recurrence
Abstract
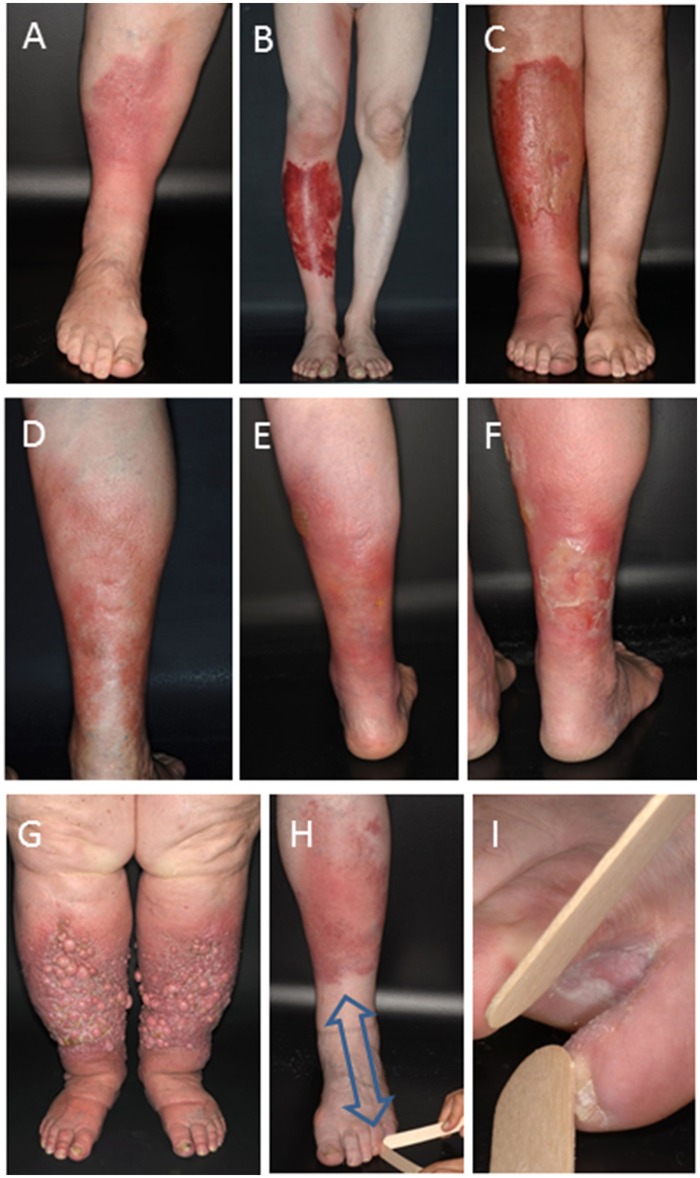
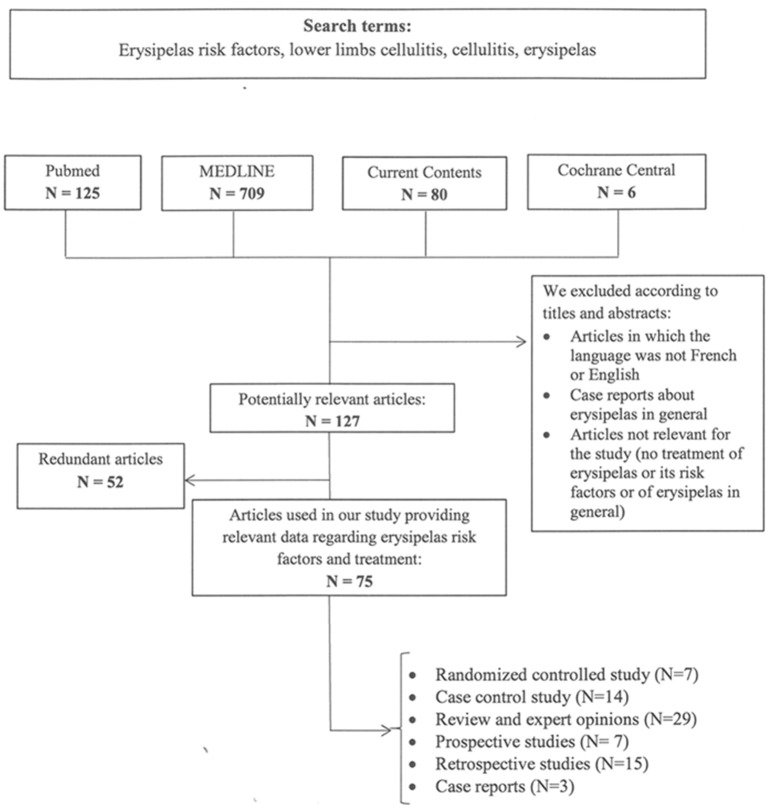
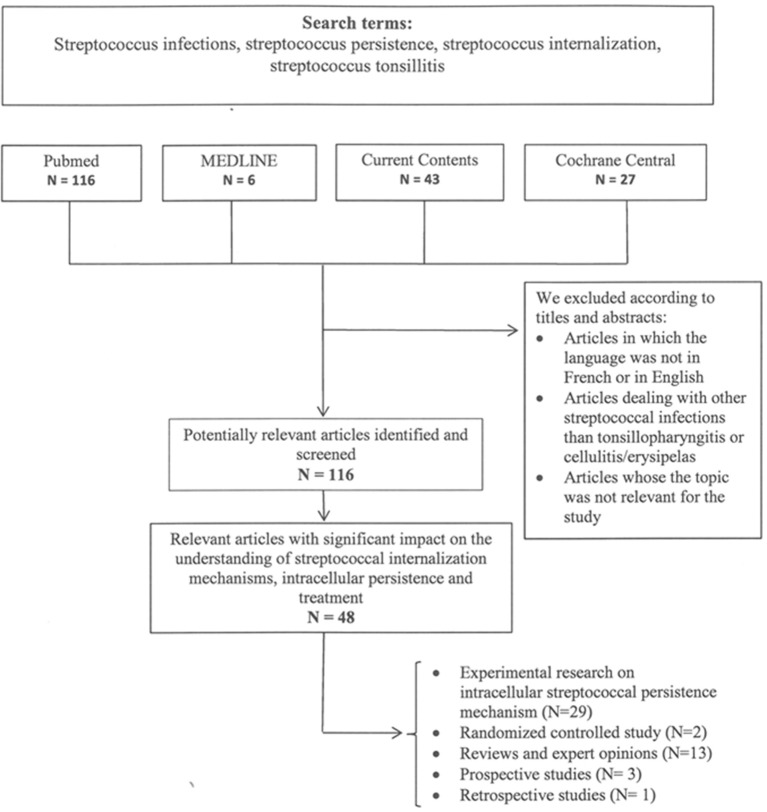
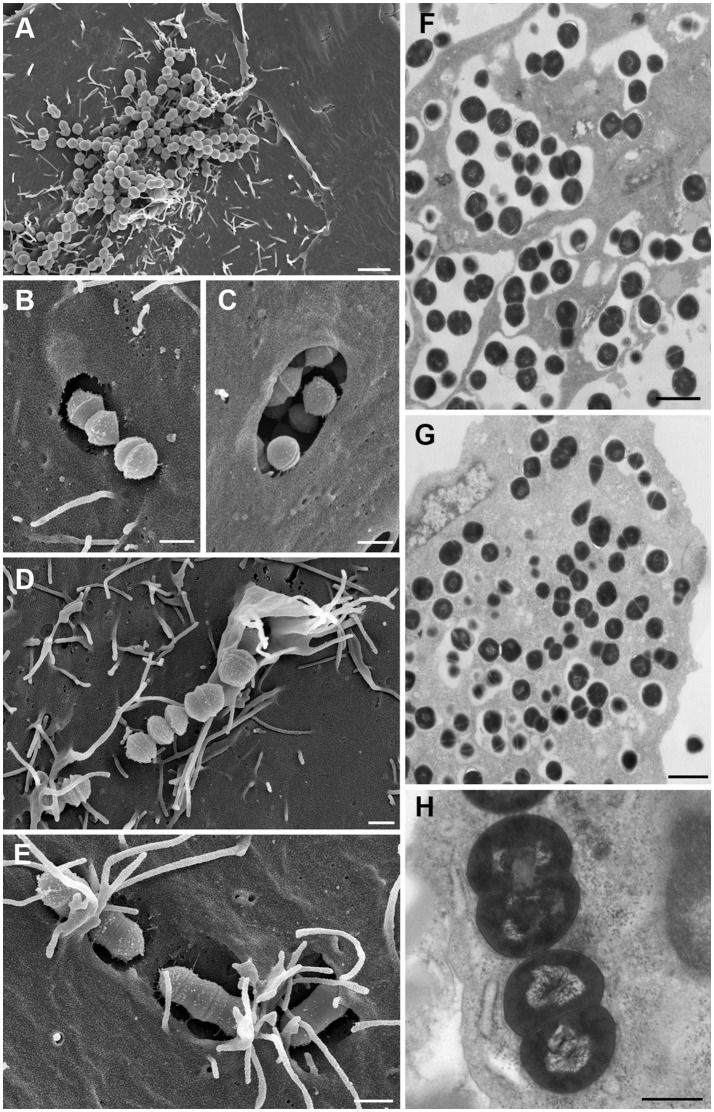
Erysipelas is a severe streptococcal infection of the skin primarily spreading through the lymphatic vessels. Penicillin is the treatment of choice. The most common complication consists in relapses which occur in up to 40% or more of patients despite appropriate antibiotic treatment. They cause lymphatic damage resulting in irreversible lymphedema and ultimately elephantiasis nostras and lead to major health restrictions and high socio-medical costs. Prevention of relapses is an unmet need, because even long-term prophylactic penicillin application does eventually not reduce the risk of recurrence. In this article we assess risk factors and causes of erysipelas recurrence. A systematic literature search for clinical studies addressing potential causes and measures for prevention of erysipelas recurrence was combined with a review of experimental and clinical data assessing the ability and clinical relevance of streptococci for intracellular uptake and persistence. The literature review found that venous insufficiency, lymphedema, and intertrigo from fungal infections are considered to be major risk factors for recurrence of erysipelas but cannot adequately explain the high recurrence rate. As hitherto unrecognized likely cause of erysipelas relapses we identify the ability of streptococci for intracellular uptake into and persistence within epithelial and endothelial cells and macrophages. This creates intracellular streptococcal reservoirs out of reach of penicillins which do not reach sufficient bactericidal intracellular concentrations. Incomplete streptococcal elimination due to intracellular streptococcal persistence has been observed in various deep tissue infections and is considered as cause of relapsing streptococcal pharyngitis despite proper antibiotic treatment. It may also serves as endogenous infectious source of erysipelas relapses. We conclude that the current antibiotic treatment strategies and elimination of conventional risk factors employed in erysipelas management are insufficient to prevent erysipelas recurrence. The reactivation of streptococcal infection from intracellular reservoirs represents a plausible explanation for the frequent occurrence erysipelas relapses. Prevention of erysipelas relapses therefore demands for novel antibiotic strategies capable of eradicating intracellular streptococcal persistence.
Keywords: cellulitis; erysipelas; intracellular streptococcal persistence; intracellular streptococcal uptake; penicillin prophylaxis; relapse; risk factors; treatment.
Figures
References
-
- Stevens DL, Bryant AE. Impetigo, erysipelas and cellulitis. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations. Oklahoma City, OK: University of Oklahoma Health Sciences Center; (2016). p. 723–40. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials