

Neprilysin inhibition for pulmonary arterial hypertension: a randomized, double-blind, placebo-controlled, proof-of-concept trial
- PMID: 30761523
- PMCID: PMC7651846
- DOI: 10.1111/bph.14621
Neprilysin inhibition for pulmonary arterial hypertension: a randomized, double-blind, placebo-controlled, proof-of-concept trial
Abstract
Background and purpose: Pulmonary arterial hypertension (PAH) is an incurable, incapacitating disorder resulting from increased pulmonary vascular resistance, pulmonary arterial remodelling, and right ventricular failure. In preclinical models, the combination of a PDE5 inhibitor (PDE5i) with a neprilysin inhibitor augments natriuretic peptide bioactivity, promotes cGMP signalling, and reverses the structural and haemodynamic deficits that characterize PAH. Herein, we conducted a randomized, double-blind, placebo-controlled trial to assess the efficacy and safety of repurposing the neprilysin inhibitor, racecadotril, in PAH.
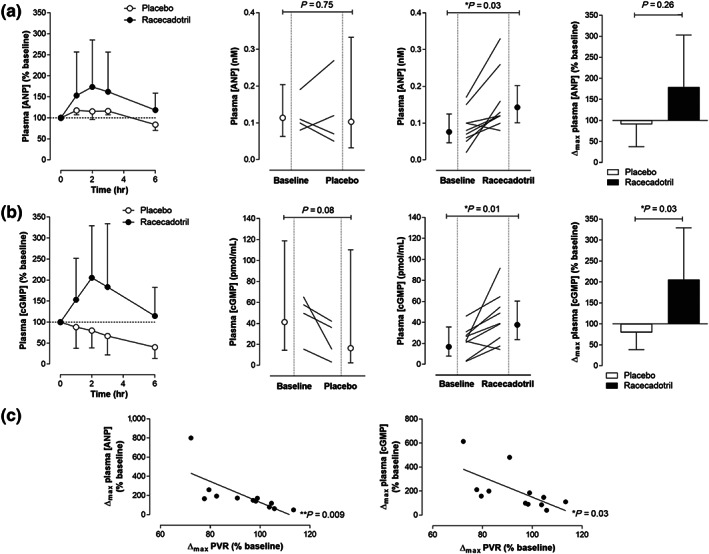
Experimental approach: Twenty-one PAH patients stable on PDE5i therapy were recruited. Acute haemodynamic and biochemical changes following a single dose of racecadotril or matching placebo were determined; this was followed by a 14-day safety and efficacy evaluation. The primary endpoint in both steps was the maximum change in circulating atrial natriuretic peptide (ANP) concentration (Δmax ), with secondary outcomes including pulmonary and systemic haemodynamics plus mechanistic biomarkers.
Key results: Acute administration of racecadotril (100 mg) resulted in a 79% increase in the plasma ANP concentration and a 106% increase in plasma cGMP levels, with a concomitant 14% fall in pulmonary vascular resistance. Racecadotril (100 mg; t.i.d.) treatment for 14 days resulted in a 19% rise in plasma ANP concentration. Neither acute nor chronic administration of racecadotril resulted in a significant drop in mean arterial BP or any serious adverse effects.
Conclusions and implications: This Phase IIa evaluation provides proof-of-principle evidence that neprilysin inhibitors may have therapeutic utility in PAH and warrants a larger scale prospective trial.
© 2019 The British Pharmacological Society.
Conflict of interest statement
B.S. has been a consultant/advisory board member for GSK & Actelion. J.C. has been a consultant/advisory board member for Actelion, GSK, Bayer, United Therapeutics, Endotronic, and Pfizer. A.H. has been a consultant/advisory board member for Bayer AG, Serodus ASA, and Palatin Technologies Inc.
Figures





Similar articles
-
Selonsertib in adults with pulmonary arterial hypertension (ARROW): a randomised, double-blind, placebo-controlled, phase 2 trial.Lancet Respir Med. 2022 Jan;10(1):35-46. doi: 10.1016/S2213-2600(21)00032-1. Epub 2021 Aug 20. Lancet Respir Med. 2022. PMID: 34425071 Clinical Trial.
-
Switching to riociguat versus maintenance therapy with phosphodiesterase-5 inhibitors in patients with pulmonary arterial hypertension (REPLACE): a multicentre, open-label, randomised controlled trial.Lancet Respir Med. 2021 Jun;9(6):573-584. doi: 10.1016/S2213-2600(20)30532-4. Epub 2021 Mar 24. Lancet Respir Med. 2021. PMID: 33773120 Clinical Trial.
-
Additive protective effects of sacubitril/valsartan and bosentan on vascular remodelling in experimental pulmonary hypertension.Cardiovasc Res. 2021 Apr 23;117(5):1391-1401. doi: 10.1093/cvr/cvaa200. Cardiovasc Res. 2021. PMID: 32653925
-
Phosphodiesterase 5 inhibitors for pulmonary hypertension.Cochrane Database Syst Rev. 2019 Jan 31;1(1):CD012621. doi: 10.1002/14651858.CD012621.pub2. Cochrane Database Syst Rev. 2019. PMID: 30701543 Free PMC article.
-
Evidence-based pharmacologic management of pulmonary arterial hypertension.Clin Ther. 2007 Oct;29(10):2134-53. doi: 10.1016/j.clinthera.2007.10.009. Clin Ther. 2007. PMID: 18042471 Review.
Cited by
-
Clinical Characteristics and Outcomes of Patients With Heart Failure With Reduced Ejection Fraction and Chronic Obstructive Pulmonary Disease: Insights From PARADIGM-HF.J Am Heart Assoc. 2021 Feb 16;10(4):e019238. doi: 10.1161/JAHA.120.019238. Epub 2021 Jan 30. J Am Heart Assoc. 2021. PMID: 33522249 Free PMC article. Clinical Trial.
-
Cyclic GMP and PKG Signaling in Heart Failure.Front Pharmacol. 2022 Apr 11;13:792798. doi: 10.3389/fphar.2022.792798. eCollection 2022. Front Pharmacol. 2022. PMID: 35479330 Free PMC article. Review.
-
Therapy for Pulmonary Arterial Hypertension: Glance on Nitric Oxide Pathway.Front Pharmacol. 2021 Nov 12;12:767002. doi: 10.3389/fphar.2021.767002. eCollection 2021. Front Pharmacol. 2021. PMID: 34867394 Free PMC article. Review.
-
Treatment of Pulmonary Hypertension With Angiotensin II Receptor Blocker and Neprilysin Inhibitor Sacubitril/Valsartan.Circ Heart Fail. 2019 Nov;12(11):e005819. doi: 10.1161/CIRCHEARTFAILURE.119.005819. Epub 2019 Nov 11. Circ Heart Fail. 2019. PMID: 31707802 Free PMC article.
-
New and Emerging Therapeutic Drugs for the Treatment of Pulmonary Arterial Hypertension: A Systematic Review.Cureus. 2024 Aug 29;16(8):e68117. doi: 10.7759/cureus.68117. eCollection 2024 Aug. Cureus. 2024. PMID: 39347150 Free PMC article. Review.
References
-
- Ando, S. , Rahman, M. A. , Butler, G. C. , Senn, B. L. , & Floras, J. S. (1995). Comparison of candoxatril and atrial natriuretic factor in healthy men. Effects on hemodynamics, sympathetic activity, heart rate variability, and endothelin. Hypertension, 26, 1160–1166. 10.1161/01.HYP.26.6.1160 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
