

Technical Note: Simplified and practical pretherapy tumor dosimetry - A feasibility study for 131 I-MIBG therapy of neuroblastoma using 124 I-MIBG PET/CT
- PMID: 30761545
- PMCID: PMC6510622
- DOI: 10.1002/mp.13446
Technical Note: Simplified and practical pretherapy tumor dosimetry - A feasibility study for 131 I-MIBG therapy of neuroblastoma using 124 I-MIBG PET/CT
Abstract
Purpose: Radiation dose calculated on tumors for radiopharmaceutical therapy varies significantly from tumor to tumor and from patient to patient. Accurate estimation of radiation dose requires multiple time point measurements using radionuclide imaging modalities such as SPECT or PET. In this report, we show our technical development of reducing the number of scans needed for reasonable estimation of tumor and normal organ dose in our pretherapy imaging and dosimetry platform of 124 I-metaiodobenzylguanidine (MIBG) positron emission tomography/computed tomography (PET/CT) for 131 I-MIBG therapy of neuroblastoma.
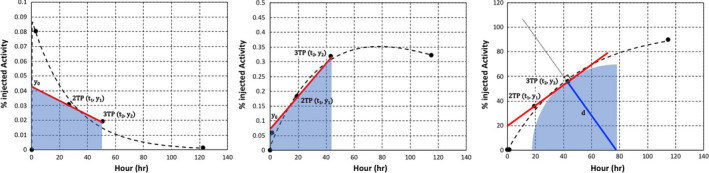
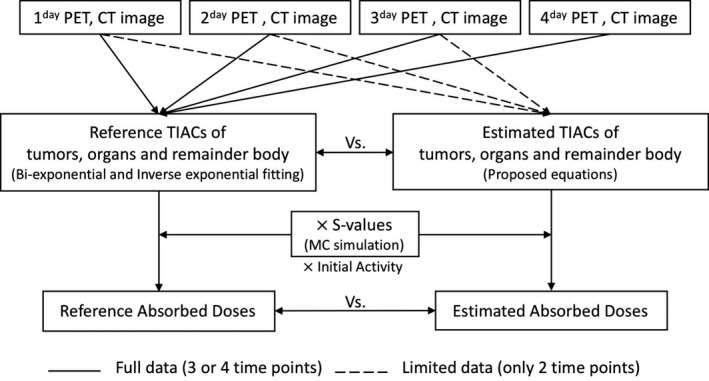
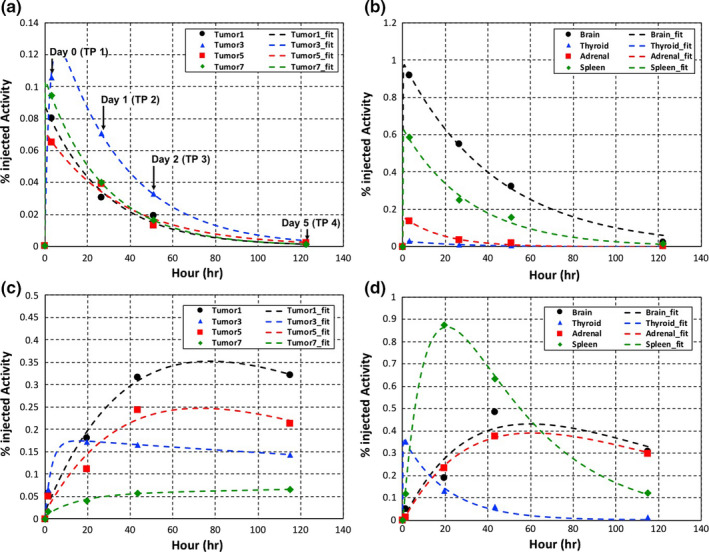
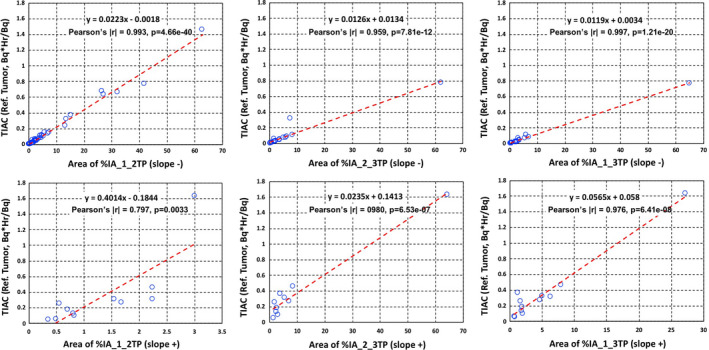
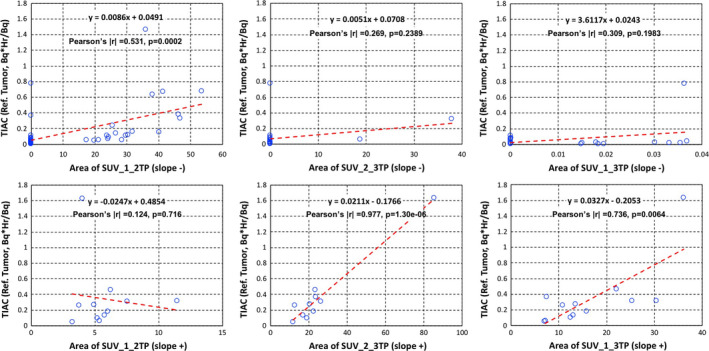
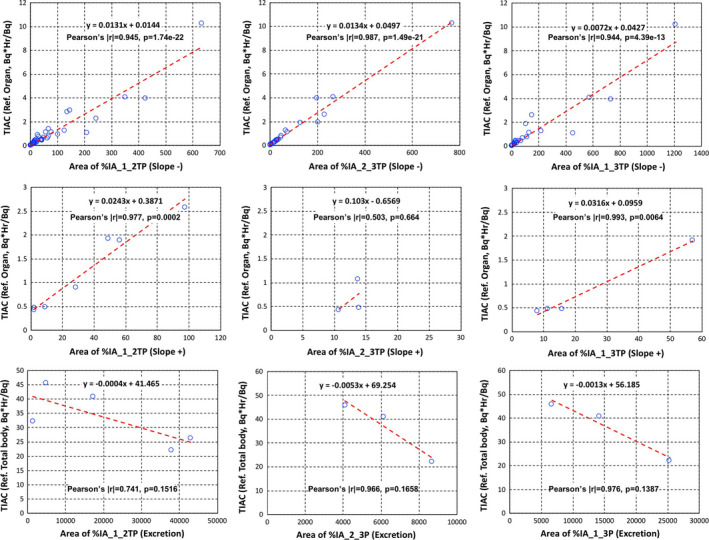
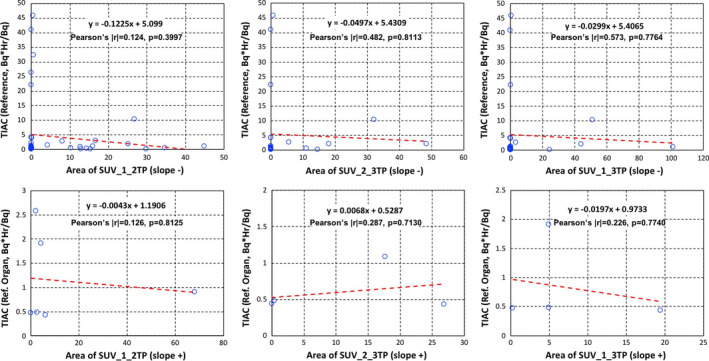
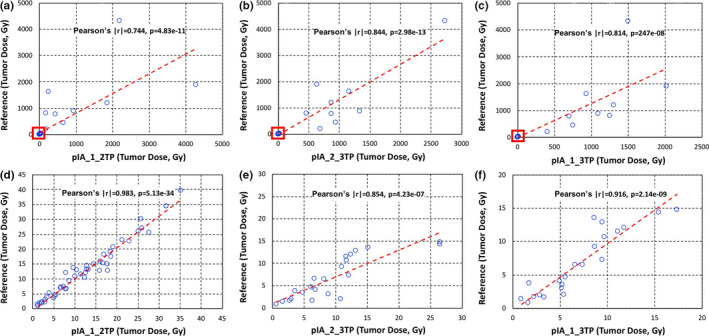
Methods: We analyzed the simplest kinetic data, areas of two-time point data for five patients with neuroblastoma who underwent 3 or 4 times of 124 I-MIBG PET/CT scan prior to 131 I-MIBG therapy. The data for which we derived areas were percent of injected activity (%IA) and standardized uptake value of tumors. These areas were correlated with time-integrated activity coefficients (TIACs) from full data (3 or 4 time points). TIACs are direct correlates with radiation dose as long as the volume and the radionuclide are known.
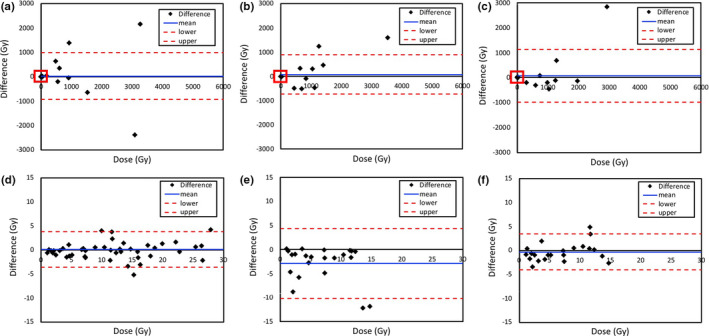
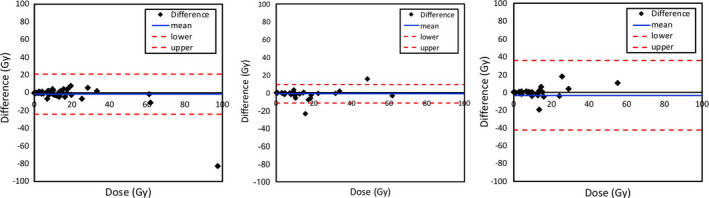
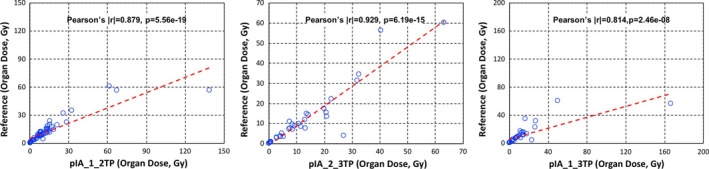
Results: The areas of %IAs between data obtained from all the two-time points with time points 1 and 2 (day 0 and day 1), time points 2 and 3 (day 1 and day 2), and time points 1 and 3 (day 0 and day 2) showed reasonable correlation (Pearson's correlation coefficient |r| > 0.5) with not only tumor and organ TIACs but also tumor and organ absorbed doses. The tumor and organ doses calculated using %IA areas of time point 1 and time point 2 were our best fits at about 20% individual percent difference compared to doses calculated using 3 or 4 time points.
Conclusions: We could achieve reasonable accuracy of estimating tumor doses for subsequent radiopharmaceutical therapy using only the two-time point imaging sessions. Images obtained from these time points (within the 48-h after administration of radiopharmaceutical) were also viewed as useful for diagnostic reading. Although our analysis was specific to 124 I-MIBG PET/CT pretherapy imaging data for 131 I-MIBG therapy of neuroblastoma and the number of imaging datasets was not large, this feasible methodology would generally be applicable to other imaging and therapeutic radionuclides with an appropriate data analysis similar to our analysis to other imaging and therapeutic radiopharmaceuticals.
Keywords: MIBG; dosimetry; neuroblastoma; radionuclide therapy; tumor dosimetry.
© 2019 American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no conflict to disclose.
Figures
References
-
- Matthay KK, Panina C, Huberty J, et al. Correlation of tumor and whole‐body dosimetry with tumor response and toxicity in refractory neuroblastoma treated with (131)I‐MIBG. J Nucl Med. 2001;42:1713–1721. - PubMed
-
- Sgouros G, Kolbert KS, Sheikh A, et al. Patient‐specific dosimetry for 131I thyroid cancer therapy using 124I PET and 3‐dimensional‐internal dosimetry (3D‐ID) software. J Nucl Med. 2004;45:1366–1372. - PubMed
-
- Sgouros G, Squeri S, Ballangrud AM, et al. Patient‐specific, 3‐dimensional dosimetry in non‐Hodgkin's lymphoma patients treated with 131I‐anti‐B1 antibody: assessment of tumor dose‐response. J Nucl Med. 2003;44:260–268. - PubMed
