

Diuretic Resistance in Heart Failure
- PMID: 30762178
- PMCID: PMC6431570
- DOI: 10.1007/s11897-019-0424-1
Diuretic Resistance in Heart Failure
Abstract
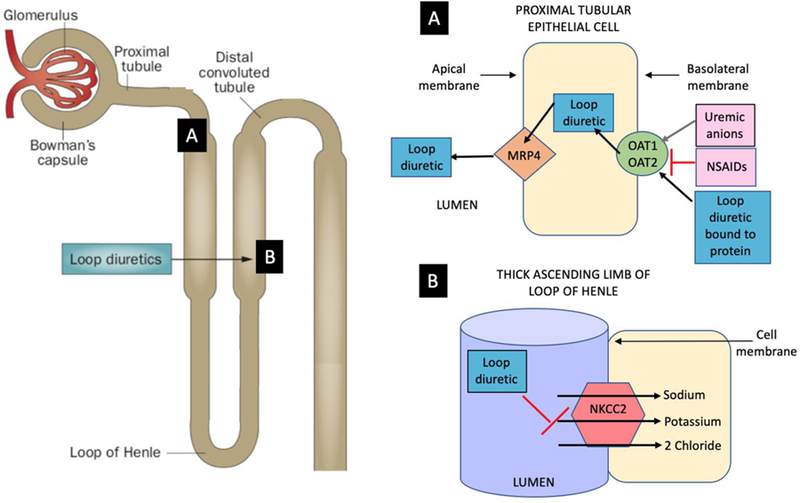
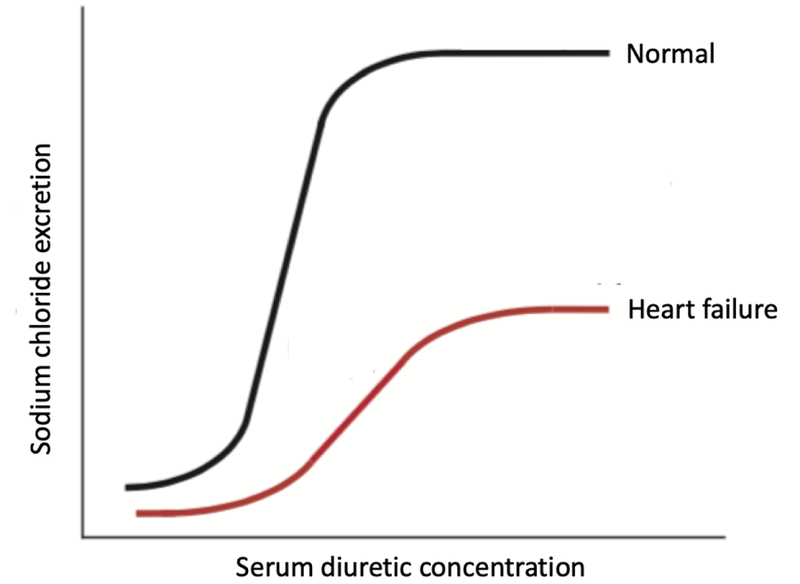
Purpose of review: Diuretic resistance (DR) occurs along a spectrum of relative severity and contributes to worsening of acute heart failure (AHF) during an inpatient stay. This review gives an overview of mechanisms of DR with a focus on loop diuretics and summarizes the current literature regarding the prognostic value of diuretic efficiency and predictors of natriuretic response in AHF.
Recent findings: The pharmacokinetics of diuretics are impaired in chronic heart failure, but little is known about mechanisms of DR in AHF. Almost all diuresis after administration of a loop diuretic dose occurs in the first few hours after administration and within-dose DR can develop. Recent studies suggest that DR at the level of the nephron may be more important than defects in diuretic delivery to the tubule. Because loop diuretics induce natriuresis, urine sodium (UNa) concentration may serve as a functional, physiological, and direct measure for diuretic responsiveness to a given loop diuretic dose. Identifying and targeting individuals with DR for more aggressive, tailored therapy represents an important opportunity to improve outcomes. A better understanding of the mechanistic underpinnings of DR in AHF is needed to identify additional biomarkers and guide future trials and therapies.
Keywords: Acute heart failure; Biomarkers; Diuretic resistance; Loop diuretics; Spot urine sodium.
Conflict of interest statement
Conflict of Interest
Richa Gupta declares no conflicts of interest.
Figures
References
-
- Wang H, Dwyer-Lindgren L, Lofgren KT, Rajaratnam JK, Marcus JR, Levin-Rector A, et al. Age-specific and sex-specific mortality in 187 countries, 1970–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013;380:2071–94. - PubMed
-
- Ambrosy AP, Pang PS, Khan S, Konstam MA, Fonarow GC, Traver B, et al. Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: findings from the EVEREST trial. Eur Heart J 2013;34:835–43. - PubMed
-
- Gheorghiade M, Follath F, Ponikowski P, Barsuk JH, Blair JE, Cleland JG, et al. Assessing and grading congestion in acute heart failure: a scientific statement from the acute heart failure committee of the Heart Failure Association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur J Heart Fail 2010;12:423–33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
