

Patient-Reported Outcomes One to Five Years After Anterior Cruciate Ligament Reconstruction: The Effect of Combined Injury and Associations With Osteoarthritis Features Defined on Magnetic Resonance Imaging
- PMID: 30762314
- PMCID: PMC6693993
- DOI: 10.1002/acr.23854
Patient-Reported Outcomes One to Five Years After Anterior Cruciate Ligament Reconstruction: The Effect of Combined Injury and Associations With Osteoarthritis Features Defined on Magnetic Resonance Imaging
Abstract
Objective: Persistent symptoms and poor quality of life (QoL) are common following anterior cruciate ligament reconstruction (ACLR). We aimed to determine the influence of a combined ACL injury (i.e., concomitant meniscectomy and/or arthroscopic chondral defect at the time of ACLR and/or secondary injury/surgery to ACLR knee) and cartilage defects defined on magnetic resonance imaging (MRI), bone marrow lesions (BMLs), and meniscal lesions on patient-reported outcomes 1 to 5 years after ACLR.
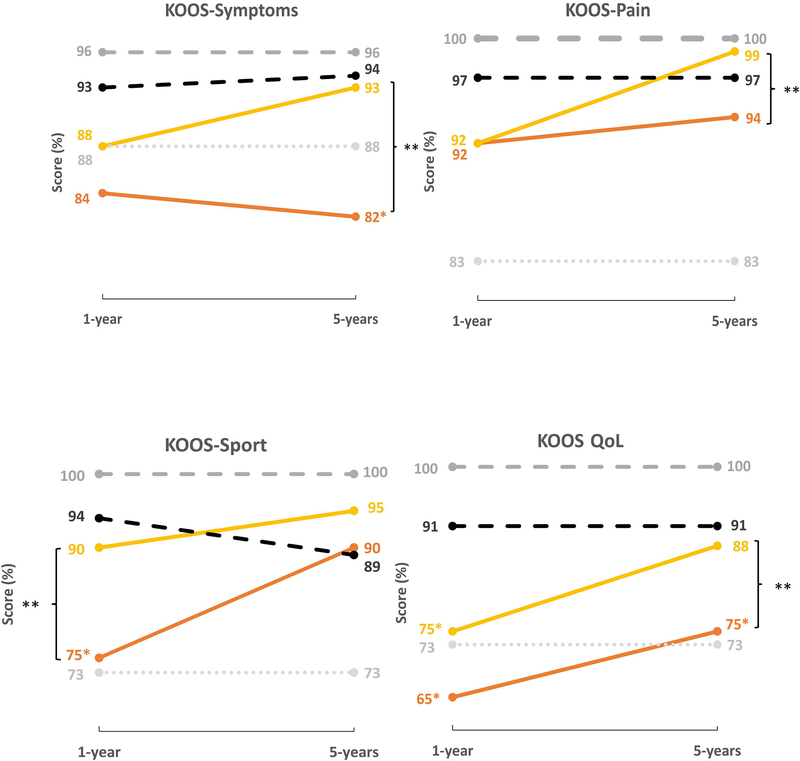
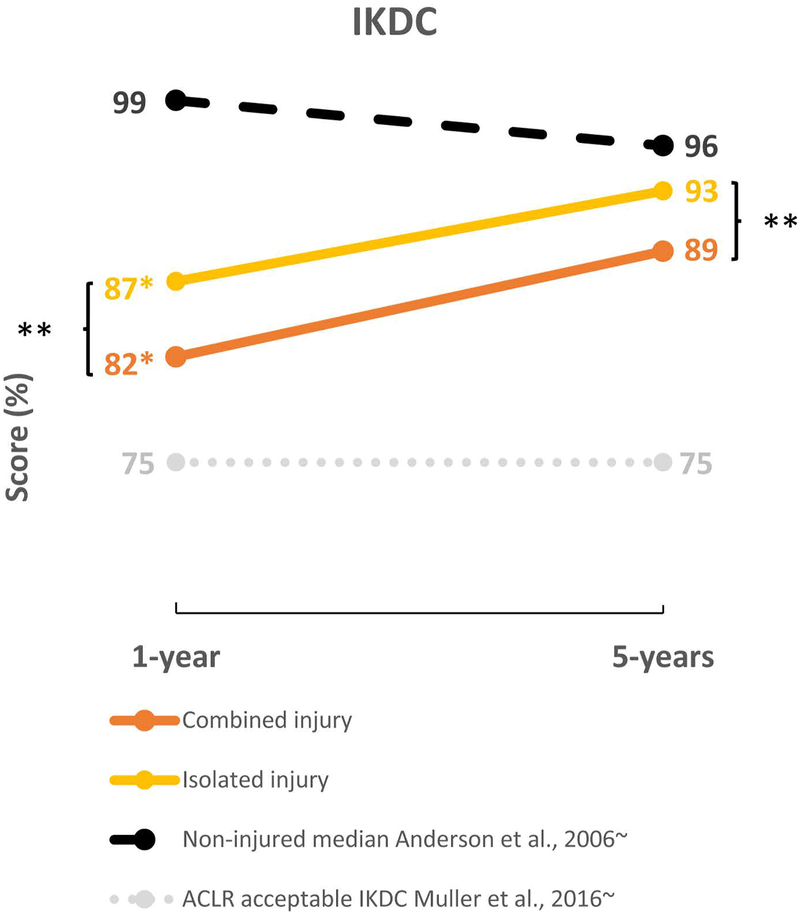
Methods: A total of 80 participants (50 men; mean ± SD age 32 ± 14 years) completed the Knee Injury and Osteoarthritis Outcome Score (KOOS) and the International Knee Documentation Committee (IKDC) questionnaires as well as a 3T MRI assessment at 1 and 5 years after ACLR. Median patient-reported outcome scores were compared between isolated and combined ACL injuries and with published normative values. Using multivariate regression, we evaluated the association between compartment-specific MRI cartilage, BMLs, and meniscal lesions and patient-reported outcomes at 1 and 5 years.
Results: Individuals with a combined injury had significantly worse scores in the KOOS subscale of function in sport and recreation (KOOS sport/rec) and in the IKDC questionnaire at 1 year, and worse scores in the KOOS subscales of pain (KOOS pain), symptoms (KOOS symptoms), and QoL (KOOS QoL) and in the IKDC questionnaire at 5 years compared to those with an isolated injury. Although no feature on MRI was associated with patient-reported outcomes cross-sectionally at 1 year, patellofemoral cartilage defects at 1 year were significantly associated with worse 5-year KOOS symptoms (β = -9.79, 95% confidence interval [95% CI] -16.67, -2.91), KOOS sport/rec (β = -7.94, 95% CI -15.27, -0.61), KOOS QoL (β = -8.29, 95% CI -15.28, -1.29), and IKDC (β = -4.79, 95% CI -9.34, -0.24) scores. Patellofemoral cartilage defects at 5 years were also significantly associated with worse 5-year KOOS symptoms (β = -6.86, 95% CI -13.49, -0.24) and KOOS QoL (β = -11.71, 95% CI -19.08, -4.33) scores.
Conclusion: Combined injury and patellofemoral cartilage defects shown on MRI are associated with poorer long-term outcomes. Clinicians should be vigilant and aware of individuals with these injuries, as such individuals may benefit from targeted interventions to improve QoL and optimize symptoms.
© 2019, American College of Rheumatology.
Conflict of interest statement
Potential conflict of interest:
Ali Guermazi is a shareholder of Boston Imaging Core Lab (BICL), LLC, and a consultant to MerckSerono, Pfizer, GE Healthcare, Galapagos, Roche and TissueGene. No other authors declare a conflict of interest.
Figures

Similar articles
-
Poor functional performance 1 year after ACL reconstruction increases the risk of early osteoarthritis progression.Br J Sports Med. 2020 May;54(9):546-553. doi: 10.1136/bjsports-2019-101503. Epub 2020 Apr 10. Br J Sports Med. 2020. PMID: 32276925
-
Early Patellofemoral Osteoarthritis Features One Year After Anterior Cruciate Ligament Reconstruction: Symptoms and Quality of Life at Three Years.Arthritis Care Res (Hoboken). 2016 Jun;68(6):784-92. doi: 10.1002/acr.22761. Arthritis Care Res (Hoboken). 2016. PMID: 26473410
-
Patients With Concomitant Intra-articular Lesions at Index Surgery Deteriorate in Their Knee Injury and Osteoarthritis Outcome Score in the Long Term More Than Patients With Isolated Anterior Cruciate Ligament Rupture: A Study From the Swedish National Anterior Cruciate Ligament Register.Arthroscopy. 2018 May;34(5):1520-1529. doi: 10.1016/j.arthro.2017.11.019. Epub 2018 Feb 1. Arthroscopy. 2018. PMID: 29395549
-
Lysholm and KOOS QoL Demonstrate High Responsiveness in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Randomized Clinical Trials.Am J Sports Med. 2024 Oct;52(12):3161-3166. doi: 10.1177/03635465231219966. Epub 2024 Feb 14. Am J Sports Med. 2024. PMID: 38352999
-
Single-stage repair of displaced bucket-handle meniscal tears with anterior cruciate ligament reconstruction leads to good meniscal survivorship : a retrospective cohort study.Bone Joint J. 2022 Jun;104-B(6):680-686. doi: 10.1302/0301-620X.104B6.BJJ-2021-1340.R2. Bone Joint J. 2022. PMID: 35638209 Review.
Cited by
-
Smoking and secondary ACL rupture are detrimental to knee health post ACL injury-a Bayesian analysis.J Exp Orthop. 2023 Aug 9;10(1):79. doi: 10.1186/s40634-023-00638-4. J Exp Orthop. 2023. PMID: 37556084 Free PMC article.
-
Recruitment and baseline characteristics of young adults at risk of early-onset knee osteoarthritis after ACL reconstruction in the SUPER-Knee trial.BMJ Open Sport Exerc Med. 2024 Apr 4;10(2):e001909. doi: 10.1136/bmjsem-2024-001909. eCollection 2024. BMJ Open Sport Exerc Med. 2024. PMID: 38601122 Free PMC article.
-
The influence of body mass index on physical activity engagement following anterior cruciate ligament reconstruction: A systematic literature review.Heliyon. 2023 Nov 28;9(12):e22994. doi: 10.1016/j.heliyon.2023.e22994. eCollection 2023 Dec. Heliyon. 2023. PMID: 38125506 Free PMC article.
-
MRI-derived articular cartilage strains predict patient-reported outcomes six months post anterior cruciate ligament reconstruction.Sci Rep. 2025 Jul 1;15(1):21426. doi: 10.1038/s41598-025-05306-4. Sci Rep. 2025. PMID: 40594341 Free PMC article.
-
SUpervised exercise-therapy and Patient Education Rehabilitation (SUPER) versus minimal intervention for young adults at risk of knee osteoarthritis after ACL reconstruction: SUPER-Knee randomised controlled trial protocol.BMJ Open. 2023 Jan 18;13(1):e068279. doi: 10.1136/bmjopen-2022-068279. BMJ Open. 2023. PMID: 36657757 Free PMC article.
References
-
- Cox CL, Huston LJ, Dunn WR, Reinke EK, Nwosu SK, Parker RD, Wright RW, Kaeding CC, Marx RG, Amendola A et al.: Are articular cartilage lesions and meniscus tears predictive of IKDC, KOOS, and Marx activity level outcomes after anterior cruciate ligament reconstruction? A 6-year multicenter cohort study. Am J Sports Med 2014, 42(5):1058–1067. - PMC - PubMed
-
- Spindler KP, Huston LJ, Wright RW, Kaeding CC, Marx RG, Amendola A, Parker RD, Andrish JT, Reinke EK, Harrell FE Jr. et al: The prognosis and predictors of sports function and activity at minimum 6 years after anterior cruciate ligament reconstruction: a population cohort study. Am J Sports Med 2011, 39(2):348–359. - PMC - PubMed
-
- Ahlden M, Samuelsson K, Sernert N, Forssblad M, Karlsson J, Kartus J: The Swedish National Anterior Cruciate Ligament Register: a report on baseline variables and outcomes of surgery for almost 18,000 patients. Am J Sports Med 2012, 40(10):2230–2235. - PubMed
-
- Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS: A randomized trial of treatment for acute anterior cruciate ligament tears. N Engl J Med 2010, 363(4):331–342. - PubMed
-
- Ardern CL, Taylor NF, Feller JA, Webster KE: Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med 2014, 48(21):1543–1552. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
