

What Pain Levels Do TSA Patients Experience When Given a Long-acting Nerve Block and Multimodal Analgesia?
- PMID: 30762694
- PMCID: PMC6382177
- DOI: 10.1097/CORR.0000000000000597
What Pain Levels Do TSA Patients Experience When Given a Long-acting Nerve Block and Multimodal Analgesia?
Abstract
Background: The pain experience for total shoulder arthroplasty (TSA) patients in the first 2 weeks after surgery has not been well described. Many approaches to pain management have been used, with none emerging as clearly superior; it is important that any approach minimizes postoperative opioid use.
Questions/purposes: (1) With a long-acting nerve block and comprehensive multimodal analgesia, what are the pain levels after TSA from day of surgery until postoperative day (POD) 14? (2) How many opioids do TSA patients take from the day of surgery until POD 14? (3) What are the PainOUT responses at POD 1 and POD 14, focusing on side effects from opioids usage?
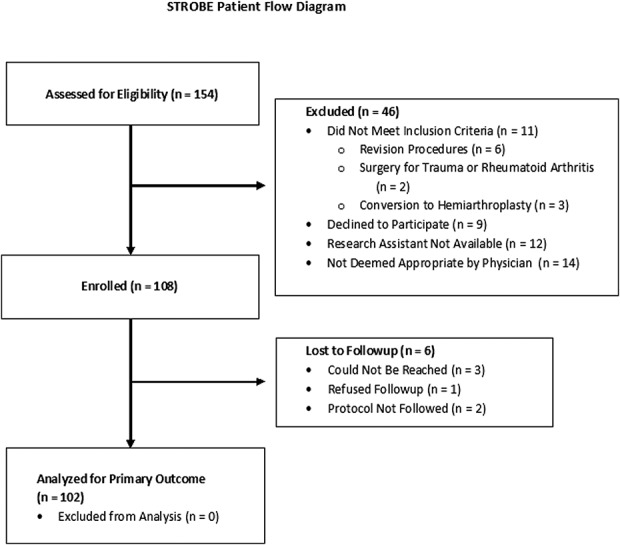
Methods: From January 27, 2017 to December 6, 2017, 154 TSA patients were identified as potentially eligible for this prospective, institutional review board-approved observational study. Of those, 46 patients (30%) were excluded (either because they were deemed not appropriate for the study, research staff were not available, patients were not eligible, or they declined to participate), and another six (4%) had incomplete followup data and could not be studied, leaving 102 patients (66%) for analysis here. Median preoperative pain with movement was 7 (interquartile range [IQR], 5-9) and 13 of 102 patients used preoperative opioids. All patients received a single-injection bupivacaine interscalene block with adjuvant clonidine, dexamethasone, and buprenorphine. Multimodal analgesia included acetaminophen, NSAIDs, and opioids. The primary outcome was the Numerical Rating Scale (NRS) pain score with movement on POD 14. The NRS pain score ranges from 0 (no pain) to 10 (worst pain possible). Secondary outcomes included NRS pain scores at rest and with movement (day of surgery, and PODs 1, 3, 7 and 14), daily analgesic use from day of surgery to POD 14 (both oral and intravenous), Opioid-Related Symptom Distress Scale (which assesses 12 symptoms ranging from 0 to 4, with 4 being the most distressing; the composite score is the mean of the 12 symptom-specific scores) on POD 1, and the PainOut questionnaire on POD 1 and POD 14. The PainOut questionnaire includes questions rating nausea, drowsiness, itching from 0 (none) to 10 (severe), as well as rating difficulty staying asleep from 0 (does not interfere) to 10 (completely interferes).
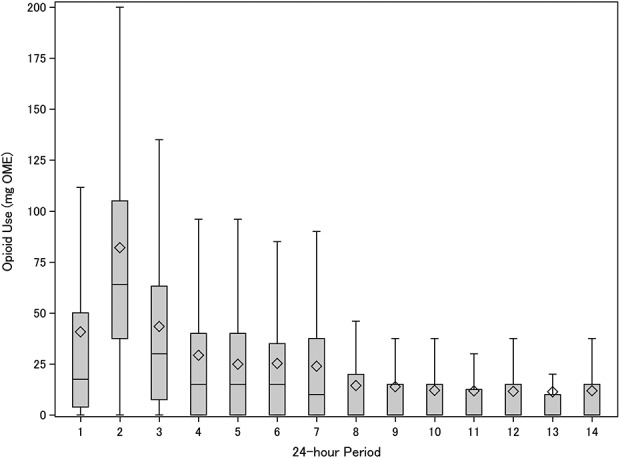
Results: The median NRS pain scores with movement were 2 (IQR, 0-5) on POD 1, 5 (IQR, 3-6) on POD 3, and the pain score was 3 (IQR, 1-5) on POD 14. Median total opioid use (converted to oral morphine equivalents) was 16 mg (4-50 mg) for the first 24 hours, 30 mg (8-63 mg) for the third, and 0 mg (0-20 mg) by the eighth 24-hour period, while the most frequent number of activations of the intravenous patient-controlled analgesia device was 0. Median PainOut scores on POD 1 and POD 14 for sleep interference, nausea, drowsiness and itching were 0, and the median composite Opioid-Related Symptom Distress Scale score on day 1 was 0.3 (IQR, 0.1-0.5).
Conclusions: Clinicians using this protocol, which combines a long-acting, single-injection nerve block with multimodal analgesia, can inform TSA patients that their postoperative pain will likely be less than their preoperative pain, and that on average they will stop using opioids after 7 days. Future research could investigate what the individual components of this protocol contribute. Larger cohort studies or registries would document the incidence of rare complications. Randomized controlled trials could directly compare analgesic effectiveness and cost-benefits for this protocol versus alternative strategies, such as perineural catheters or liposomal bupivacaine. Perhaps most importantly, future studies could seek ways to further reduce peak pain and opioid usage on POD 2 and POD 3.
Level of evidence: Level IV, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures


Comment in
-
CORR Insights®: What Pain Levels Do TSA Patients Experience When Given a Long-acting Nerve Block and Multimodal Analgesia?Clin Orthop Relat Res. 2019 Mar;477(3):633-634. doi: 10.1097/CORR.0000000000000670. Clin Orthop Relat Res. 2019. PMID: 30762695 Free PMC article. No abstract available.
References
-
- Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52:69-77. - PubMed
-
- Breivik H, Borchgrevink PC, Allen SM, Rosseland LA, Romundstad L, Hals EK, Kvarstein G, Stubhaug A. Assessment of pain. Br J Anaesth. 2008;101:17-24. - PubMed
-
- Brummett CM, Janda AM, Schueller CM, Tsodikov A, Morris M, Williams DA, Clauw DJ. Survey criteria for fibromyalgia independently predict increased postoperative opioid consumption after lower-extremity joint arthroplasty: a prospective, observational cohort study. Anesthesiology. 2013;119:1434-1443. - PMC - PubMed
-
- Bryan NA, Swenson JD, Greis PE, Burks RT. Indwelling interscalene catheter use in an outpatient setting for shoulder surgery: technique, efficacy, and complications. J Shoulder Elbow Surg. 2007;16:388-395. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
