

Pneumocystis jirovecii pneumonia as an initial manifestation of hyper-IgM syndrome in an infant: A case report
- PMID: 30762803
- PMCID: PMC6408131
- DOI: 10.1097/MD.0000000000014559
Pneumocystis jirovecii pneumonia as an initial manifestation of hyper-IgM syndrome in an infant: A case report
Abstract
Rationale: Pneumocystis jirovecii causes severe pneumonia in immunocompromised hosts. Human immunodeficiency virus infection, malignancy, solid organ or hematopoietic cell transplantation, and primary immune deficiency compose the risk factors for Pneumocystis pneumonia (PCP) in children, and PCP can be an initial clinical manifestation of primary immune deficiency.
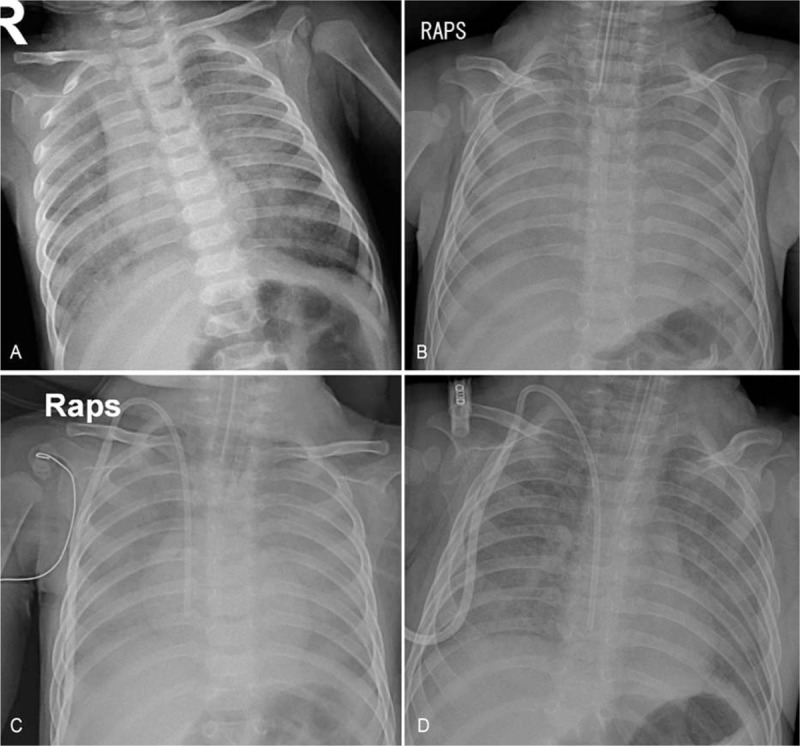
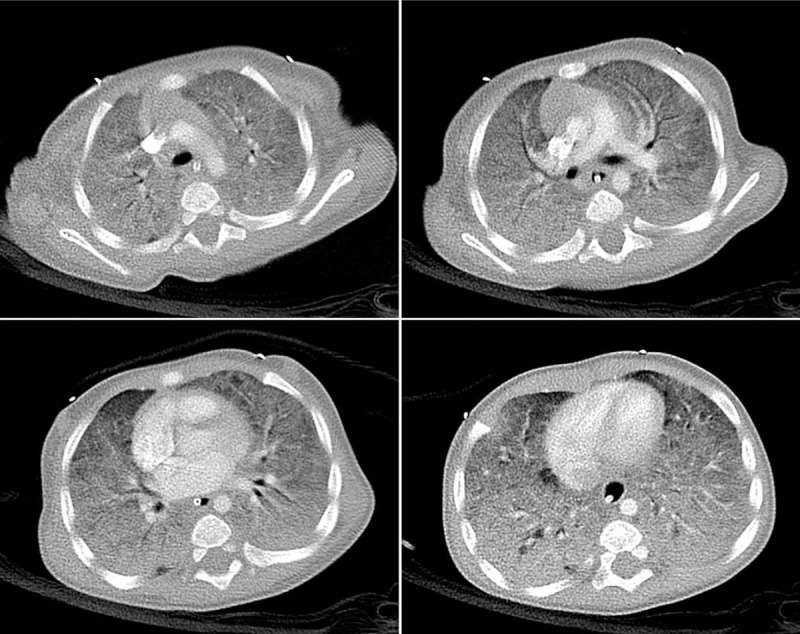
Patient concerns: A 5-month-old infant presented with cyanosis and tachypnea. He had no previous medical or birth history suggesting primary immune deficiency. He was diagnosed with interstitial pneumonia on admission.
Diagnoses: He was diagnosed with PCP, and further evaluations revealed underlying X-linked hyper-IgM syndrome.
Interventions: He was treated with trimethoprim/sulfamethoxazole for PCP, and eventually received allogeneic hematopoietic cell transplantation for hyper-IgM syndrome.
Outcomes: Twenty months have passed after transplantation without severe complications.
Lessons: PCP should be considered in infants presenting with severe interstitial pneumonia even in the absence of evidence of immune deficiency. Primary immune deficiency should also be suspected in infants diagnosed with PCP.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Interstitial pneumonia as the initial presentation in an infant with a novel mutation of CD40 ligand-associated X-linked hyper-IgM syndrome: A case report.Medicine (Baltimore). 2020 Jun 12;99(24):e20505. doi: 10.1097/MD.0000000000020505. Medicine (Baltimore). 2020. PMID: 32541472 Free PMC article.
-
X-Linked Hyper IgM Syndrome Manifesting as Recurrent Pneumocystis jirovecii Pneumonia: A Case Report.J Trop Pediatr. 2020 Dec 1;66(6):648-654. doi: 10.1093/tropej/fmaa023. J Trop Pediatr. 2020. PMID: 32388558
-
Diagnosis and treatment of Pneumocystis jirovecii pneumonia in HIV-infected or non-HIV-infected patients-difficulties in diagnosis and adverse effects of trimethoprim-sulfamethoxazole.J Infect Chemother. 2019 Nov;25(11):920-924. doi: 10.1016/j.jiac.2019.06.007. Epub 2019 Jul 9. J Infect Chemother. 2019. PMID: 31300379
-
[Pneumocystis jirovecii pneumonia-an opportunistic infection undergoing change].Internist (Berl). 2019 Jul;60(7):669-677. doi: 10.1007/s00108-019-0616-5. Internist (Berl). 2019. PMID: 31089770 Review. German.
-
Clinical, Diagnostic, and Treatment Disparities between HIV-Infected and Non-HIV-Infected Immunocompromised Patients with Pneumocystis jirovecii Pneumonia.Respiration. 2018;96(1):52-65. doi: 10.1159/000487713. Epub 2018 Apr 10. Respiration. 2018. PMID: 29635251 Review.
Cited by
-
Human-Fungal Pathogen Interactions from the Perspective of Immunoproteomics Analyses.Int J Mol Sci. 2024 Mar 20;25(6):3531. doi: 10.3390/ijms25063531. Int J Mol Sci. 2024. PMID: 38542504 Free PMC article. Review.
-
A novel CD40LG mutation causing X‑linked hyper-IgM syndrome.Glob Med Genet. 2024 Nov 20;12(3):100007. doi: 10.1016/j.gmg.2024.100007. eCollection 2025 Sep. Glob Med Genet. 2024. PMID: 40330326 Free PMC article.
-
Detection of Pneumocystis jirovecii in Hospitalized Children Less Than 3 Years of Age.J Fungi (Basel). 2021 Jul 9;7(7):546. doi: 10.3390/jof7070546. J Fungi (Basel). 2021. PMID: 34356925 Free PMC article.
-
Pneumocystis Pneumonia: Immunity, Vaccines, and Treatments.Pathogens. 2021 Feb 19;10(2):236. doi: 10.3390/pathogens10020236. Pathogens. 2021. PMID: 33669726 Free PMC article. Review.
-
Of Mycelium and Men: Inherent Human Susceptibility to Fungal Diseases.Pathogens. 2023 Mar 14;12(3):456. doi: 10.3390/pathogens12030456. Pathogens. 2023. PMID: 36986378 Free PMC article. Review.
References
-
- Goldman AS, Goldman LR, Goldman DA. What caused the epidemic of Pneumocystis pneumonia in European premature infants in the mid-20th century? Pediatrics 2005;115:e725–36. - PubMed
-
- Catherinot E, Lanternier F, Bougnoux ME, et al. Pneumocystis jirovecii pneumonia. Infect Dis Clin North Am 2010;24:107–38. - PubMed
-
- Saltzman RW, Albin S, Russo P, et al. Clinical conditions associated with PCP in children. Pediatr Pulmonol 2012;47:510–6. - PubMed
-
- Elenga N, Dulorme F, de Saint Basile G, et al. Pneumocystis jiroveci pneumonia revealing de novo mutation causing X-linked hyper-IgM syndrome in an infant male. The first case reported from French Guiana. J Pediatr Hematol Oncol 2012;34:528–30. - PubMed
-
- Heinold A, Hanebeck B, Daniel V, et al. Pitfalls of “hyper”-IgM syndrome: a new CD40 ligand mutation in the presence of low IgM levels. A case report and a critical review of the literature. Infection 2010;38:491–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
