

Comparative pathophysiology and management of protein-losing enteropathy
- PMID: 30762910
- PMCID: PMC6430879
- DOI: 10.1111/jvim.15406
Comparative pathophysiology and management of protein-losing enteropathy
Abstract
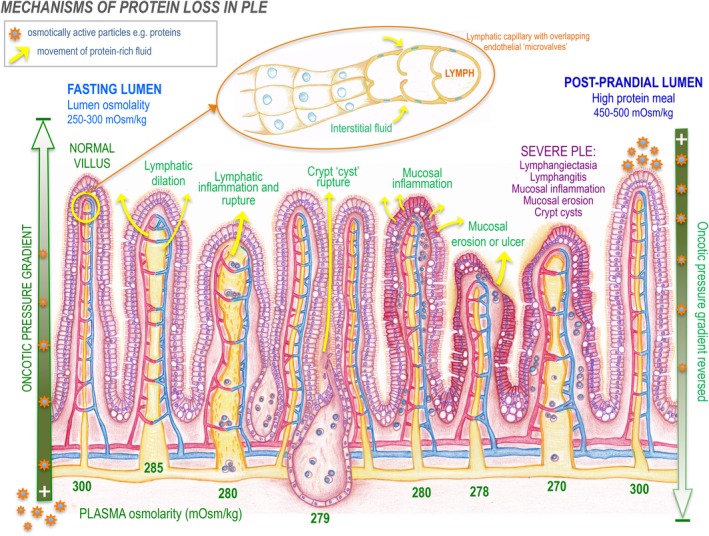
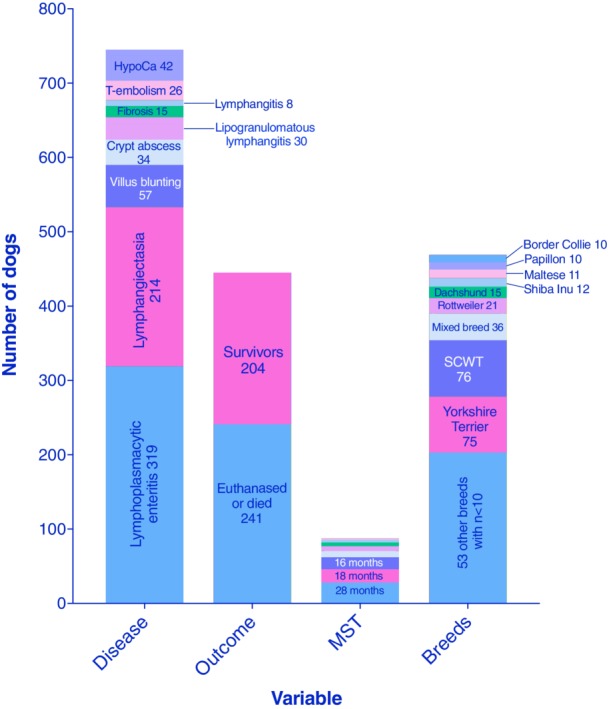
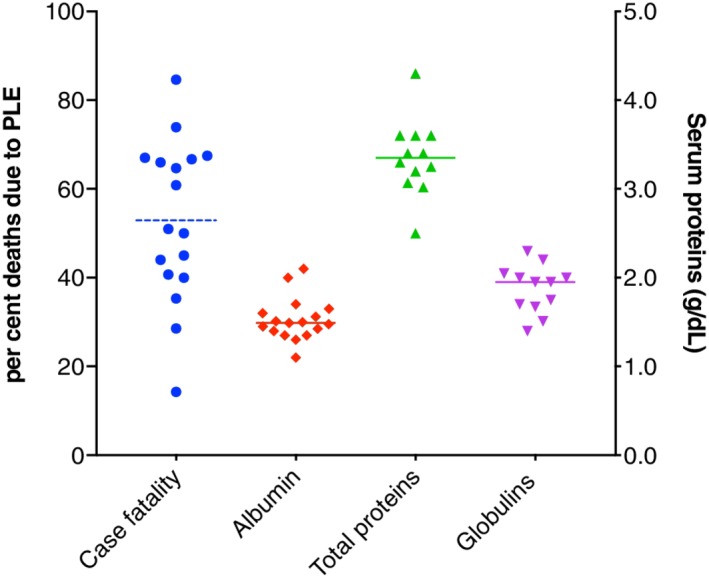
Protein-losing enteropathy, or PLE, is not a disease but a syndrome that develops in numerous disease states of differing etiologies and often involving the lymphatic system, such as lymphangiectasia and lymphangitis in dogs. The pathophysiology of lymphatic disease is incompletely understood, and the disease is challenging to manage. Understanding of PLE mechanisms requires knowledge of lymphatic system structure and function, which are reviewed here. The mechanisms of enteric protein loss in PLE are identical in dogs and people, irrespective of the underlying cause. In people, PLE is usually associated with primary intestinal lymphangiectasia, suspected to arise from genetic susceptibility, or "idiopathic" lymphatic vascular obstruction. In dogs, PLE is most often a feature of inflammatory bowel disease (IBD), and less frequently intestinal lymphangiectasia, although it is not proven which process is the true driving defect. In cats, PLE is relatively rare. Review of the veterinary literature (1977-2018) reveals that PLE was life-ending in 54.2% of dogs compared to published disease-associated deaths in IBD of <20%, implying that PLE is not merely a continuum of IBD spectrum pathophysiology. In people, diet is the cornerstone of management, whereas dogs are often treated with immunosuppression for causes of PLE including lymphangiectasia, lymphangitis, and crypt disease. Currently, however, there is no scientific, extrapolated, or evidence-based support for an autoimmune or immune-mediated mechanism. Moreover, people with PLE have disease-associated loss of immune function, including lymphopenia, severe CD4+ T-cell depletion, and negative vaccinal titers. Comparison of PLE in people and dogs is undertaken here, and theories in treatment of PLE are presented.
Keywords: PLE; crypt; hypoalbuminemia; lymphangiectasia; lymphatic; panhypoproteinemia.
© 2019 The Authors. Journal of Veterinary Internal Medicine published by Wiley Periodicals, Inc. on behalf of the American College of Veterinary Internal Medicine.
Conflict of interest statement
Authors declare no conflict of interest.
Figures


References
-
- Rovenská E, Rovenský J. Lymphatic vessels: structure and function. Isr Med Assoc J. 2011;13(12):762‐768. - PubMed
-
- Waldmann TA, Steinfeld JL, Dutcher TF, Davidson JD, Gordon RS. The role of the gastrointestinal system in idiopathic hypoproteinemia. Gastroenterology. 1961;41:197‐207. - PubMed
-
- Takeda H, Ishihama K, Fukui T, et al. Significance of rapid turnover proteins in protein‐losing gastroenteropathy. Hepatogastroenterology. 2003;50(54):1963‐1965. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
